

The genesis of the INTREPID Transformer I/A Handpiece (Alcon) was based on my experience with coaxial and bimanual irrigation and aspiration. The former is what most residents and fellows learn in their training, and the latter I learned when I left training and went into practice.
In the United States, surgeons tend to favor coaxial removal of cortex in cataract surgery, while the bimanual technique is more popular in Europe. Although each approach produces excellent outcomes, circumstances—sometimes arising quickly mid-case—often dictate choosing one over the other.
Coaxial vs Bimanual: Each Has Its Place
Speed has become an important factor for cataract surgeons, and one of the advantages of coaxial irrigation and aspiration is that, in my experience, the cortex is removed quickly and efficiently at higher flow and vacuum settings (Figure 1).
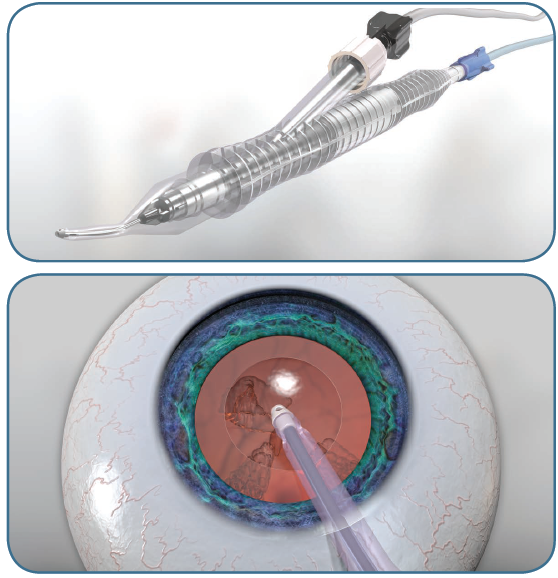
Figure 1. Advantages of coaxial irrigation and aspiration (see video).
Bimanual surgery, achieved by separating the inflow from the vacuum aspiration, is a slower, more controlled technique. With two points of entry into the eye, you also have more control of the eye as you manipulate it to perform certain parts of the procedure (Figure 2). At the same time, irrigation inflow and aspiration outflow can by varied, which is desirable in certain cases. If a patient cannot maintain fixation, for example, you have more control with two instruments in the eye. If loose zonules are present or there is some disruption of the zonules, such as in a pseudoexfoliation or trauma case, you can decrease irrigation inflow and the aspiration to avoid unzippering more zonules in a “low flow” system.
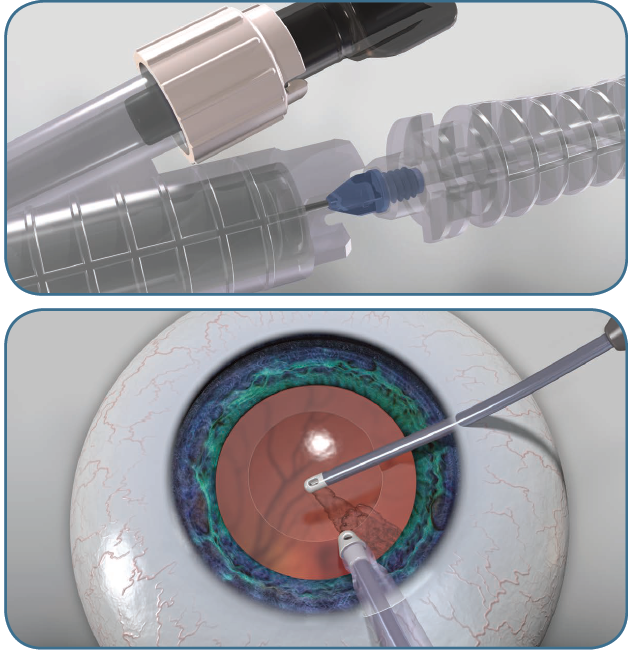
Figure 2. Bimanual surgery is achieved by separating the inflow from the vacuum aspiration.
Because bimanual surgery employs a lower flow system, I have found that the vitreous does not become overhydrated with fluid through the openings in the zonules. You can direct the irrigation into the intact bag in the area where the zonular compromise has occurred while continuing to maintain adequate IOP while removing the cortex with better control.
Furthermore, the subincisional area is more accessible with a bimanual approach, because you can change the angle at which you access that area with your aspirating port.
Why a 2-in-1 Handpiece?
Having used a bimanual technique for cortical removal for many years, I felt it would be advantageous to have a single handpiece that could be used for both coaxial and bimanual surgery to avoid all of the manipulations involved in switching from one mode to the other. This includes:
- coming out of the eye with the coaxial cannula and removing the tubing
- obtaining the bimanual instruments if they are not already on the tray
- plugging the tubing into the bimanual cannulas
- reinserting them into the eye
- because of the different irrigation gauges, possibly changing the machine parameters to obtain a lower vacuum and a lower flow setting.
These steps take time, and we do not necessarily have the luxury of time during a complicated case. Being able to simply come out of the eye, twist a single instrument, and go back into the eye with two cannulas without changing the settings provides the advantages of using two hands from two entry points into the eye, accessing areas that are not as easily accessed with a coaxial handpiece and using very low flow if indicated. It gives the surgeon the best of both worlds.
Ease of Use
Several aspects of bimanual surgery enhance safety and the ease with which we can complete procedures. For example, the bimanual technique does not require the same amount of irrigation fluid flowing into the eye to maintain the chamber as coaxial surgery does. Consequently, in my experience, the settings can be lowered significantly, lessening the potential to aspirate the capsule and tear zonules when working in the subincisional area. If you are trying to reach the subincisional area, it is much easier to come from the side to access the area beneath the primary incision site than to come from straight underneath. I think ophthalmic surgeons have been challenged by subincisional cortex from time to time, and bimanual I/A is a safer, easier option.
Shorten Your Learning Curve
Having used bimanual technique throughout my career, my learning curve was minimal. One difference I noticed is that the two access points are about 90° apart as opposed to approximately 160° apart, which I am accustomed with traditional bimanual I/A. This affects some of the control of a bimanual system. If operating temporally and that is where your primary incision is, nothing prevents you from going inferiorly (at the 3 o’clock or 9 o’clock position, depending on whether you are operating in the right or left eye), which would enable you to better control the eye. Usually, it is more convenient and somewhat easier to go more toward the side, 45° to 75°, for example, away from the incision site to access that subincisional area as well as others.
I do think there is a learning curve for surgeons who have never used bimanual technique, but it is not a difficult learning curve. It is a matter of learning how to use both hands and to switch back and forth between the two hands, because you have the ability to place sideport incisions in two different locations (Figure 3). When operating at 9 o’clock, for example, you can place a sideport paracentesis incision to your right and to your left for the aspiration cannula. I routinely do this as it provides broader access to the subincisional area should I want it.

Figure 3. During bimanual mode, the irrigation sleeve remains in the primary incision while the polymer-tipped aspiration port is used in a secondary incision.
Incision Placement
The placement of paracentesis incisions varies from surgeon to surgeon. I suggest letting your dominant hand fall where it is comfortable next to the eye, and that is the point where you may enter it. Some surgeons may be more comfortable placing the paracentesis farther away from the primary incision, while others may prefer to place it closer toward the primary incision.
Use the hand position that is most comfortable for you to use as your access point, but as you enter the eye with the paracentesis or sideport knife, angle it toward the primary incision. This enables you to maintain the integrity of the paracentesis without stretching the primary incision by having to torque the aspirating cannula of the bimanual cannula.
Advantage of Polymer Tips
I have been an advocate of the polymer tip since its introduction several years ago, mainly because it is consistently smooth compared with a metal tip.
Metal tips can be damaged during procedures or during cleaning and sterilizing, particularly within the orifice at the tip. Sharp barbs or imperfections along that inner opening can tear the capsule during polishing, particularly when you are working underneath the capsule and cannot visualize it entirely. You could unknowingly grab the capsule and tear it, creating a complication in an otherwise uncomplicated case.
The polymer tip virtually eliminates these risks, because it is an exquisitely manufactured disposable, single-use instrument.
Impact of a Dual-Duty Handpiece
The INTREPID Transformer I/A Handpiece, with its disposable, single-use polymer tip, has tremendous advantages, as it gives the surgeon the flexibility and option to use it as either a coaxial or a bimanual instrument.
Even if you are planning to use the bimanual option only occasionally, it is always ready to go right away without excessive manipulations or the use of other instruments, and without the need to change tubing and settings. It enables surgeons to use two different types of instrument in one, simplifying the procedure and improving safety while giving the surgeon a number of options.