
Sponsored By


My team and I first used the CENTURION Vision System (Alcon) approximately 2 years ago. My primary interest in switching to the CENTURION Vision System from the INFINITI Vision System (Alcon) was the fluidics.1,2 The INFINITI Vision System advanced the management of ultrasonic energy via the OZil Torsional Handpiece, 2006 (Alcon). The CENTURION Vision System builds on the ultrasonic capabilities of the INFINITI System (namely, OZil torsional ultrasound and Intelligent Phaco [IP; Alcon]) and incorporates ACTIVE FLUIDICS.1,2 I now use the CENTURION Vision System almost exclusively; it is available at four out of five of the facilities in which I operate.
SURGICAL PARAMETERS
Surgeons do not necessarily need to adjust their surgical parameters to use the CENTURION Vision System, although I have adjusted mine and will continue to do so in order to take full advantage of the levels of customization available on this phaco machine. The CENTURION Vision System has so much subtlety and so many levels of adjustability that, if you wish, you can customize every step in every phase of the procedure, which is what I prefer to do. Customized procedural templates can be created to address various surgical situations such as the highly myopic case presented herein.
At present, for most of my cases, I target a reduced IOP of between 25 and 40 mm Hg, depending on the density of the cataract and the stability of the eye. I still use linear mode to control both aspiration flow rate and vacuum, and now with the CENTURION, I can vary these parameters separately in foot positions 2 and 3. With the efficiency of the INTREPID Balanced Tip (Alcon),3,4 I have been able to reduce my torsional ultrasonic power in foot position 3 from a previous maximum of 100% to a maximum of 60%,† even for very dense nuclei. (Alcon recommends that OZil amplitude be limited to 60% for the Balanced Tip.) I have found that torsional ultrasound with OZil IP is consistently advantageous over a combination of longitudinal and torsional ultrasound.
IOP RAMP ON CENTURION VISION SYSTEM
A fluidics feature that I find particularly valuable on the CENTURION Vision System is the IOP ramp, a function of the system’s ACTIVE FLUIDICS that relies on monitoring aspiration flow rate, irrigation pressure, and vacuum to control the rise of the IOP as the eye is entered. I consider it a critical feature for maintaining the stability of the anterior segment in complex cataract procedures. The latest software allows for a maximum IOP ramp of 3 seconds, and I typically choose between 2 and 3 seconds for all of my surgeries.
When any phaco or I/A tip enters the eye in foot position 1, a patient may notice some discomfort due to the increase in pressure inside the eye and movement of the lens-iris diaphragm. In the case presented herein, for example, the IOP ramp is set to take 3 seconds for the pressure to rise from 20 mm Hg at baseline to 38 mm Hg. By raising the IOP ramp value, I am slowing down how quickly the anterior chamber pressurizes. I am moderating the IOP rise of the anterior chamber, which I find is critical in eyes with long axial lengths or unstable lens-iris diaphragms. This capability allows the surgeon to build the IOP faster or slower as he or she needs for each case. It is an element of customization that is unique to the CENTURION Vision System.
CASE PRESENTATION
Initial Steps
The patient was in his 60s with a refraction of -20.00 +2.25 D. The eye had a 37-mm axial length—extreme myopia—which made him an ideal candidate to take advantage of the ACTIVE FLUIDICS2 of the CENTURION Vision System.
I created the sideport incision with a 1-mm trapezoidal sideport blade and the primary incision (a 2.2-mm clear corneal incision) with a single-beveled microkeratome. I instilled DisCoVisc OVD (Alcon) in the anterior chamber, while being careful not to use too much so the eye would not overpressurize. I find DisCoVisc to be the most versatile OVD, because the triple negative charge of its chondroitin sulfate + sodium hyaluronate protects the endothelium well, it provides excellent space maintenance during IOL insertion, and DisCoVisc is easy to remove at the completion of the surgery.5
I performed all of the nucleus disassembly in this case under one setting mode (Figure 1). The IOP was fixed at 38 mm Hg with an IOP ramp of 3 seconds. An IOP of 38 mm Hg is equivalent to a bottle height of 52 cm in a gravity-based phaco system—a height at which surgeons may not have operated with previous generations of phaco machines (Figure 2). One can go lower with the CENTURION Vision System; 38 mm Hg of IOP is by no means the floor with this machine. The aspiration flow rate started at 10 mL/min and increased linearly through foot position 2 to its maximum of 27 mL/min, where I kept it throughout foot position 3. The vacuum went from zero at the onset of foot position 2 linearly to a maximum of 450 mm Hg at the beginning of foot position 3, and then it dropped to 340 mm Hg by the end of foot position 3. I used torsional ultrasound with IP, with an “on” threshold of 25% and a maximum of 60%.

Figure 1. When performing phaco chop at these fluidic levels, it is important to create a flat, vertical face deep enough in the nucleus that the phaco tip can hold the nucleus, even with little or no vacuum, as you use the chopper in a countermotion to mechanically divide the nucleus.
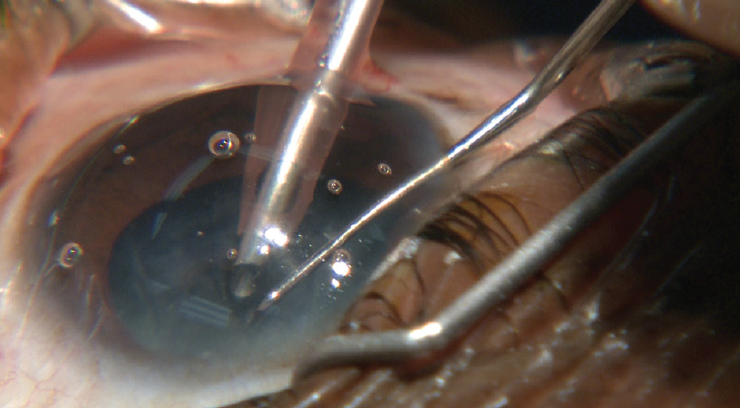
Figure 2. With the excellent fluidics of the 2.2-mm sleeve keratome system, the anterior chamber is deep, and the bag is well inflated—key features when working in the posterior or peripheral nucleus.
Capsulorhexis and Hydrodissection
The 5-mm capsulorhexis proceeded normally. With the hydrodissection, I injected BSS deliberately and gently. In a highly myopic eye such as this one, as I inject the fluid under the capsulorhexis, I simultaneously depress the posterior lip of the incision so that the viscoelastic can escape the eye as the IOP builds. In my experience, this technique prevents overpressurization and a reverse pupillary block.
Phacoemulsification
For phacoemulsification, I used the INTREPID Balanced Tip (Alcon) in a chopping technique (Figure 3). Often, when a surgeon enters a highly myopic eye like this one to perform the phacoemulsification or the I/A, the eye overpressurizes and goes into a reverse pupillary block, and the anterior chamber deepens dramatically. Then, the surgeon has to work in a much deeper anterior segment and mitigate the pupillary block. The video of this case shows how the fluidic enhancements of the CENTURION Vision System helped to prevent this from happening. This eye looked and responded like an eye of average axial length; in fact, it was remarkable how normally this eye behaved. The anterior segment remained stable throughout the entire procedure. The iris did not trampoline, and the anterior chamber did not deepen. The procedure flowed beautifully.
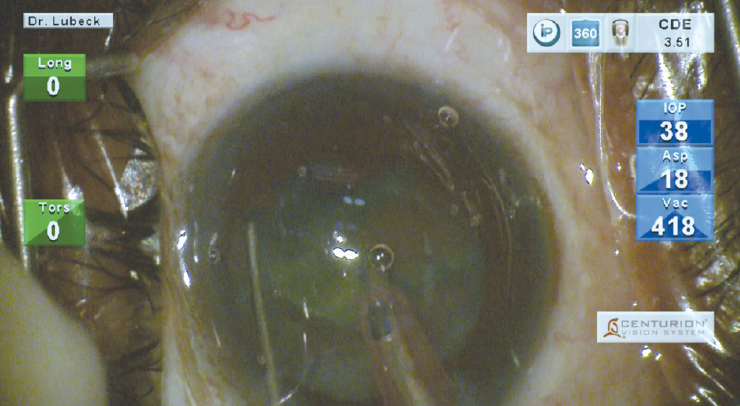
Figure 3. During quadrant removal, IP helps guide my use of torsional ultrasound. If I hear IP engaging, I will go farther down on the foot pedal, surpassing the IP needed into full torsional. Depending on the density of the cataract, it will be up to 60% torsional ultrasound power using the INTREPID Balanced Tip.
I/A With INTREPID Transformer Handpiece
I used the INTREPID Transformer I/A handpiece* (Figure 4A–C), the newest handpiece from Alcon, to first perform coaxial I/A with fluidics settings similar to traditional I/A instruments. Here, the IOP ramp was 3.0 seconds, and the IOP was 40 mm Hg. My maximum vacuum for this case was 700+ mm Hg, under linear control. The handpiece has a coaxial polymer tip that is tactile and user-friendly. The unique feature of this handpiece is that it can transform into a bimanual I/A instrument with an aspiration tip that fits through a 1-mm sideport incision. The surgeon can switch between coaxial and bimanual I/A as desired. This flexibility gives him or her better access to the subincisional cortex as well as greater maneuverability for working in an unstable anterior chamber. The INTREPID Transformer I/A system,* in conjunction with the ACTIVE FLUIDICS of the CENTURION Vision System, maintained complete stability of the anterior chamber and capsular bag during cortical removal in an otherwise challenging eye. At the conclusion of this surgery, I implanted a three-piece extended-series -5.00 D IOL (Alcon), the closest available power to the calculated ideal. The patient returned the next day with 20/40 UCVA.
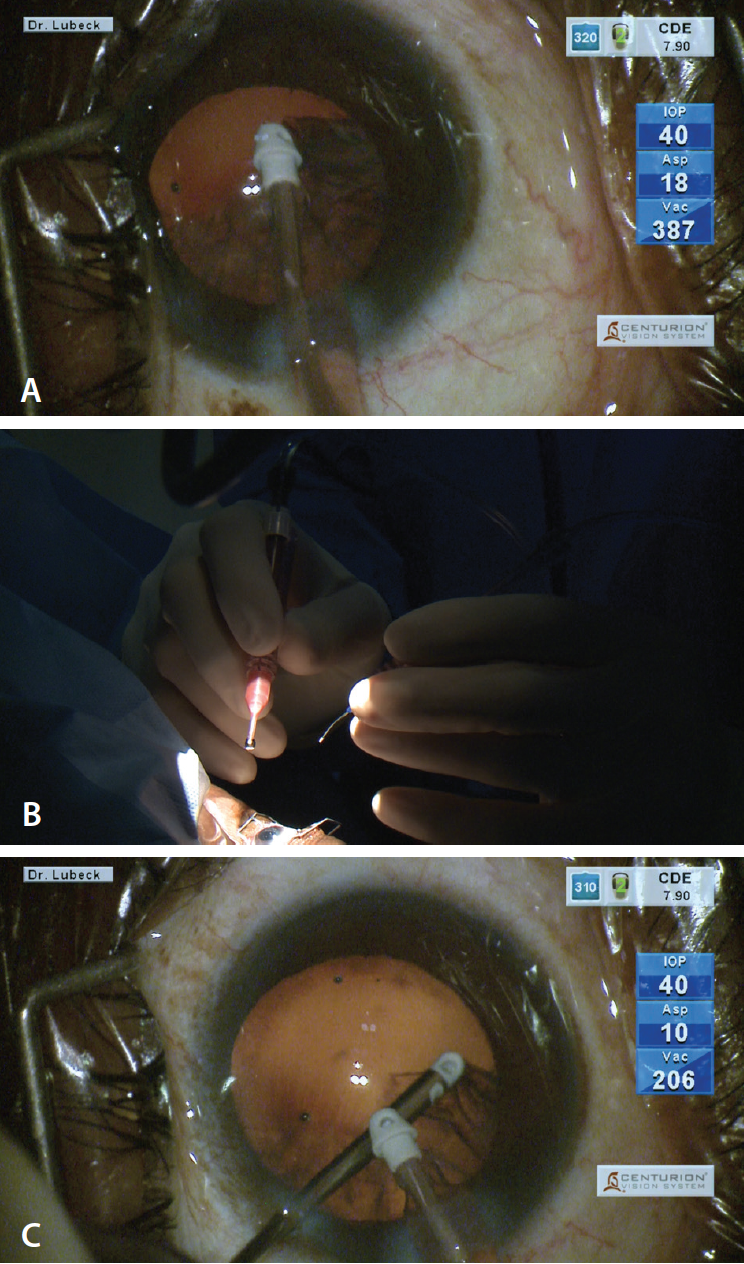
Figure 4. The Transformer I/A handpiece incorporates the benefits of a polymer tip into a system that can convert from coaxial to bimanual (A). The Transformer’s versatility allows easy access to all quadrants of the capsular bag (B). The oval aperature of the bimanual aspiration tip easily grasps cortex and small nuclear fragments (C).
I tend to use superlatives when I am describing the ACTIVE FLUIDICS of the CENTURION Vision System to colleagues and patients because, in my opinion, they are the best I have ever used on a phaco machine. In my experience, the ACTIVE FLUIDICS on the CENTURION Vision System is so adaptable that, for me, it can make difficult cases feel quite routine.
† Compared to INFINITI© Vision System and 45º Mini-Flare tip. Alcon; Fort Worth, TX.
1. Sharif-Kashani P, Fanney D, Injev V. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophthalmol. 2014;14:96.
2. Nicoli M, Miller K, Dimalanta R, Loke D: Jules Stein Institute, UCLA. IOP stability measurement and comparison between gravity-fed and actively controlled phacoemulsification systems. 2014.
3. Solomon K, Lorente R, Cionni R, Fanney D. Prospective, randomized clinical study using a new phaco system with intraocular system target pressure control. Presented at: ASCRS-ASOA Symposium and Congress; April 25-29, 2014; Boston, MA.
4. Zacharias J. Comparative motion profile characterization of the mini flared and balanced phacoemulsification tips. ESCRS; September 5-9, 2015; Barcelona, Spain.
5. DisCoVisc [package insert]. Fort Worth, TX: Alcon.
*Physicians should contact their Alcon representative about the availability of the INTREPID Transformer I/A system.