
The AcrySof IQ IOL (Alcon) is designed to provide a youthful lens to patients with cataracts. With its advanced biocompatible material and innovative design, it is designed to mimic the young adult lens by not only reducing spherical aberrations, but also filtering blue light. The design of the AcrySof IQ IOL reduced total higher-order aberrations (HOAs) and improved mesopic contrast sensitivity at 6 cpd (with and without glare) and functional vision versus the prior spherical control.1
GOLDEN OPPORTUNITY
Studies have shown that HOAs may provide some benefits, such as a natural defense against ocular chromatic aberrations2 and mitigation of image deterioration by myopic defocus.3 However, HOAs also degrade optical image quality.4,5 Due to its high refractive power, the cornea is a known primary contributor to HOAs.5,6 For instance, at a typical 6-mm pupillary diameter, the cornea contributes about +0.274 μm of spherical aberration,7 a larger portion than that of any other contributor.
In the young lens, the cornea contributes positive spherical aberration, while the crystalline lens contributes negative spherical aberration. This results in the overall spherical aberration of the eye being slightly positive. With age, physiologic changes occur in the crystalline lens, which cause the overall spherical aberration of the eye to become more positive.
When surgeons remove a cataract and implant an IOL, a golden opportunity presents itself: to use an IOL that, in my opinion, provides just the right amount of negative spherical aberration, an amount that is similar to that of a young adult's natural crystalline lens.7,8-10
optimal SPHERICAL ABERRATION
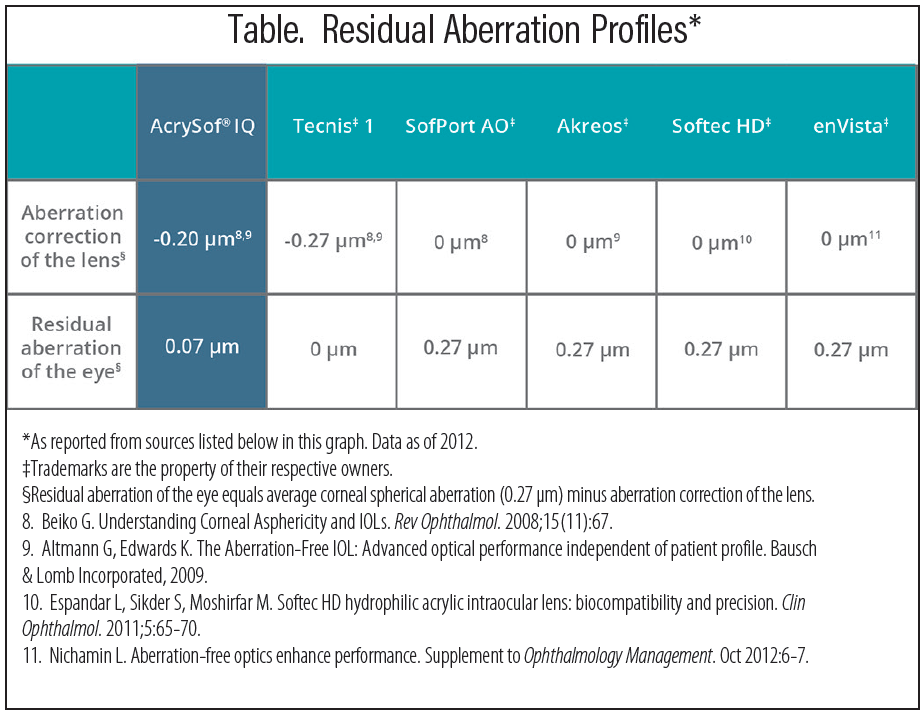
In designing the AcrySof IQ IOL, we looked at multiple studies that revealed the typical young adult human lens has an internal lens spherical aberration of -0.18 μm.6,7,9,11 Thus, we designed the AcrySof IQ IOL with a spherical aberration of -0.2 μm to give patients a modest residual positive spherical aberration (ie, ~ +0.1 μm at a 6-mm entrance pupil) (Table). This amount is consistent with that found in a young adult lens at peak visual performance,12 in US Navy pilots,13 and in a visual performance study that included young subjects.14
Providing just the right amount of spherical aberration produces excellent patient outcomes. After developing the AcrySof IQ IOL, our analysis showed that the majority of patients had the spherical aberration typical of a young adult lens.1
MATERIAL AND DESIGN
The single-piece AcrySof IQ IOL is composed of a high refractive index, soft, foldable, hydrophobic acrylic material. The AcrySof IQ IOL is available in two separate options: an ultraviolet-blocking lens and an ultraviolet and short wavelength blue light-filtering lens. Blue-light filtering chromophores were added to the AcrySof design to mimic filters in a young adult's crystalline lens. These chromophores have been shown to contribute to increase glare tolerance and functional vision versus IOLs lacking this specific chromophore.15
Design features of the AcrySof IQ IOL address surgical challenges such as achieving refractive predictability while minimizing HOAs.1 With moderate surface asphericity, the AcrySof IQ IOL helps compensate for optical degradation caused by surgical misalignments such as lens decentration and tilt.
Because of its central lens thickness of only about 0.6 mm for mid-power lenses, the AcrySof IQ IOL can be delivered via small incisions, without altering the magnitude of corneal HOAs.16 This capability is also aided by the lens material, which is appreciated for its foldability. In addition, the low rate of Nd:YAG of all AcrySof IOLs has been attributed to the AcrySof material and square-edge design.17,18
Clinical studies assessing tilt and decentration have confirmed the stability of the single-piece platform19,20 as well as the benefits of the STABLEFORCE haptic modified-L design used in the supporting haptics of the AcrySof IQ IOL.1
Calculating Optimal Spherical Aberration
Because spherical aberrations originate in both the cornea and the lens, surgeons should choose the right IOL for each patient based on the total aberrations of the cornea and the IOL. Here are a few things to remember:
- Patients with a modest positive spherical aberration (+0.1 μm) experience better vision than those with none. Young adult eyes have a small amount of positive spherical aberration, which is a result of the combination of positive sphere in the cornea and negative sphere in the lens. But as the crystalline lens ages, its spherical aberration increases.
- All eyes are different, with different levels of corneal spherical aberration. Eyes can be matched to different aspheric IOLs for optimal results. The goal is to approximate youthful vision with similar residual spherical aberration.
- The asphericity of the AcrySof IQ IOL is -2.0 μm, a number designed to net eyes with the median spherical aberration of about +0.1 μm (the optimal positive value). A modest amount of positive spherical aberration also acts as a natural defense against ocular chromatic aberrations2 and mitigates image deterioration by myopic defocus.3 The goal is to offer the benefits of reduced spherical aberration to the greatest number of people, while maintaining the IOL’s insensitivity to tilt or decentration.
CLINICAL RESULTS
Physicians worldwide rely on the proven material, innovative design, and optimal asphericity of the AcrySof IQ IOL. It provides patients with crisp and reliable vision. Since the introduction of the AcrySof IQ IOL, over 100 million of these lenses have been implanted worldwide.
Compared to spherical IOLs, the AcrySof IQ IOL has shown a significantly superior reduction of spherical and total HOAs as well as significantly superior results with mesopic contrast sensitivity at 6 cpd with and without glare.1 In the same study, night-driving simulation testing and FACT contrast sensitivity testing showed that those implanted with the AcrySof IQ IOL had better functional vision in some of the most challenging driving conditions, such as in fog and under the glare of city lights.1
Furthermore, the AcrySof IQ IOL excels. Research has shown that patients had excellent vision when surgeons targeted a residual spherical aberration of +0.1 μm rather than 0 μm following cataract surgery.1 Eyes targeted for +0.1 μm spherical aberration had improved contrast sensitivity (versus control) at 3 cpd and 6 cpd in both photopic and mesopic conditions.1
© 2019 Alcon Inc. 05/19 US-NIQ-19-E-0879
AcrySof is a trademark of Alcon. All other brand/product names are the trademarks of their respective owners.
Originally published in May 2018
1. Alcon Laboratories, Inc. Product Information: AcrySof IQ Aspheric IOL. 2010.
2. McLellan JS, Marcos S, Prieto PM, Burns SA. Imperfect optics may be the eye’s defense against chromatic blur. Nature. 2002;417:174-176.
3. Marcos S, Barbero S, Jimenez-Alfaro I. Optical quality and depth-of-field of eyes implanted with spherical and aspheric intraocular lenses. J Refract Surg. 2005;21:223-235.
4. Holladay JT, Piers PA, Koranyi G, et al. A new intraocular lens design to reduce spherical aberration of pseudophakic eyes. J Refract Surg. 2002;18:683-691.
5. Koch DD, Wang L. Custom optimization of intraocular lens asphericity. Trans Am Ophthalmol Soc. 2007;105:36-41.
6. Hong X, Zhang X. Optimizing distance image quality of an aspheric multifocal intraocular lens using a comprehensive statistical design approach. Opt Express. 2008;16:20920-20934.
7. Wang L, Dai E, Koch DD, Nathoo A. Optical aberrations of the human anterior cornea. J Cataract Refract Surg. 2003;29:1514-1521.
8. Thibos LN, Hong X, Bradley A, Cheng X. Statistical variation of aberration structure and image quality in a normal population of healthy eyes. J Opt Soc Am A Opt Image Sci Vis. 2002;19:2329-2348.
9. He JC, Gwiazda J, Thorn F, Held R. Wave-front aberrations in the anterior corneal surface and the whole eye. J Opt Soc Am A Opt Image Sci Vis. 2003;20:1155-1163.
10. Sandoval HP, Fernandez de Castro LE, Vroman DT, Solomon KD. Comparison of visual outcomes, photopic contrast sensitivity, wavefront analysis, and patient satisfaction following cataract extraction and IOL implantation: aspheric vs spherical acrylic lenses. Eye. 2007;6,1-7.
11. Kingston AC, Cox IG. Population spherical aberration: associations with ametropia, age, corneal curvature, and image quality. Clin Ophthalmol. 2013;7:933-938.
12. Levy Y, Segal O, Avni I, Zadok D. Ocular higher-order aberrations in eyes with super-normal vision. Am J Ophthalmol. 2005;139:225-228.
13. Grimson JM, Schallhorn SC, Kaupp SE. Contrast sensitivity: establishing normative data for use in screening prospective naval pilots. Aviat Space Environ Med. 2002;73:28-35.
14. Legras R, Chateau N, Charman WN. Assessment of just-noticeable differences for refractive errors and spherical aberration using visual simulation. Optom Vis Sci. 2004;81:718-728.
15. Hammond BR Jr, Renzi LM, Sachak S, Brint SF. Contralateral comparison of blue-filtering and non-blue-filtering intraocular lenses: glare disability, heterochromatic contrast, and photostress recovery. Clin Ophthalmol. 2010;4:1465-1473.
16. Marcos S, Rosales P, Llorente L, Jimenez-Alfaro I. Change in corneal aberrations after cataract surgery with 2 types of aspherical intraocular lenses. J Cataract Refract Surg. 2007;33:217-226.
17. Hancox J, Spalton D, Cleary G, et al. Fellow-eye comparison of posterior capsule opacification with AcrySof SN60AT and AF-1 YA-60BB blue-blocking intraocular lenses. J Cataract Refract Surg. 2008;34:1489-1494.
18. Hill W. Why I prefer the AcrySof IQ lens. Cataract & Refractive Surgery Today. November 2006;6(11):64-66.
19. Mutlu FM, Erdurman C, Sobaci G, Bayraktar Z. Comparison of tilt and decentration of 1-piece and 3-piece hydrophobic acrylic intraocular lens. J Cataract Refract Surg. 2005;31:343-347.
20. Hayashi K, Hayashi, H. Comparison of the stability of 1-piece and 3-piece acrylic intraocular lenses in the lens capsule. J Cataract Refract Surg. 2005;31:337-342.

AcrySof® Family of Single-Piece IOLs Important Product Information
(AcrySof® UV, AcrySof ®IQ, AcrySof® IQ Toric, AcrySof®IQ ReSTOR®, and AcrySof® IQ ReSTOR® Toric IOLs)
CAUTION: Federal law restricts these devices to sale by or on the order of a physician.
INDICATION: The family of AcrySof® single-piece intraocular lenses (IOLs) includes AcrySof® UV-absorbing IOLs (“AcrySof® UV”), AcrySof ®IQ, AcrySof ®IQ Toric® and AcrySof IQ ReSTOR® and AcrySof® IQ ReSTOR® Toric IOLs. Each of these IOLs is indicated for visual correction of aphakia in adult patients following cataract surgery. In addition, the AcrySof Toric IOLs are indicated to correct pre-existing corneal astigmatism at the time of cataract surgery. The AcrySof IQ ReSTOR IOLs are for cataract patients with or without presbyopia, who desire increased spectacle independence with a multifocal vision. All of these IOLs are intended for placement in the capsular bag.
WARNINGS/PRECAUTIONS:
General cautions for all AcrySof® and AcrySof® UV IOLs: Careful preoperative evaluation and sound clinical judgment should be used by the surgeon to decide the risk/benefit ratio before implanting any IOL in a patient with any of the conditions described in the Directions for Use that accompany each IOL. Caution should be used prior to lens encapsulation to avoid lens decentration or dislocation. Viscoelastic should be removed from the eye at the close of surgery.
Additional Cautions associated with AcrySof® IQ ReSTOR® IOLs: Some patients may experience visual disturbances and/or discomfort due to multifocality, especially under dim light conditions. A reduction in contrast sensitivity may occur in low light conditions. Visual symptoms may be significant enough that the patient will request explant of the multifocal IOL. Spectacle independence rates vary with all multifocal IOLs; as such, some patients may need glasses when reading small print or looking at small objects. Clinical studies indicate that posterior capsule opacification (PCO), when present, may develop earlier into clinically significant PCO with multifocal IOLs.
Additional Cautions associated with AcrySof® IQ Toric, AcrySof® UV Toric and ReSTOR® Toric IOLs: Optical theory suggests that, high astigmatic patients (i.e. > 2.5 D) may experience spatial distortions. Possible toric IOL related factors may include residual cylindrical error or axis misalignments. Toric IOLs should not be implanted if the posterior capsule is ruptured, if the zonules are damaged, or if a primary posterior capsulotomy is planned. Rotation can reduce astigmatic correction; if necessary lens repositioning should occur as early as possible prior to lens encapsulation.
Prior to surgery, physicians should provide prospective patients with a copy of the appropriate Patient Information Brochure available from Alcon informing them of possible risks and benefits associated with the AcrySof® IQ Toric, AcrySof® IQ ReSTOR® and AcrySof® IQ ReSTOR® Toric IOLs.
Do not resterilize. Do not store at temperatures over 45° C. Use only sterile irrigating solutions to rinse or soak IOLs.
ATTENTION: Refer to the Directions for Use labeling for the specific IOL for a complete list of indications, warnings and precautions.


