

iStent and iStent inject: How They Differ
Glaukos trabecular microbypass stents (TBS) are microinvasive glaucoma surgery (MIGS) devices used to treat primary open-angle glaucoma. iStent and iStent inject (Glaukos) were designed to lower IOP by creating a bypass through the trabecular meshwork (TM), providing a direct channel between the anterior chamber and Schlemm’s canal.
Glaukos TBS have been shown to be both effective and safe when treating mild to moderate glaucoma. The vanguard product of the MIGS revolution was the first generation iStent, which is a single stent shaped like a snorkel with retention ridges. It is made from an implant grade, heparin-coated titanium alloy and is inserted in the TM manually. With dimensions of 1 mm in length and 0.3 mm in height, the iStent was previously the smallest known medical device implanted in the human body and proved very successful in the market while helping hundreds of thousands of patients in the process.1
The second-generation model is the iStent inject, which is currently the smallest known medical device implanted in the human body (Figure 1). iStent inject comes with two stents, as opposed to the first-generation device that only came with one stent. It is similarly composed of implant-grade titanium and is 360 μm in length and 230 μm in width, which is one-third the size of the first-generation iStent. Each stent contains a central inlet and multiple outlets designed to provide multidirectional flow through Schlemm’s canal.1
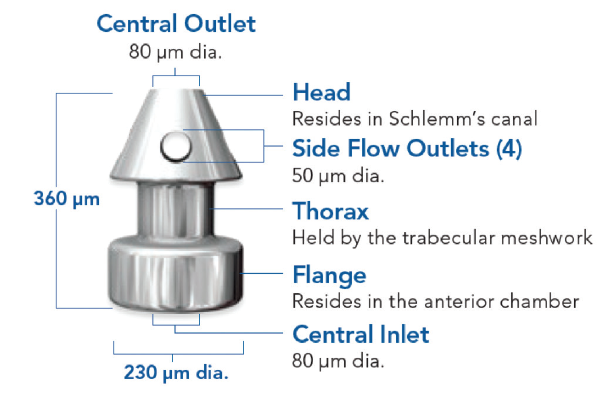
Figure 1. iStent inject dimensions.
The iStent inject removed some of the manual approach to the surgery by having two preloaded stents in one delivery system (Figure 2). Instead of visualizing the chamber in a side-to-side motion, the surgeon visualizes the TM, inserts the trocar into the TM, and presses the stent delivery button to deploy the first stent. This is repeated 2 to 3 clock hours away with the second stent. This now allows access to more collector channels, which can increase circumferential flow and further lower IOP.
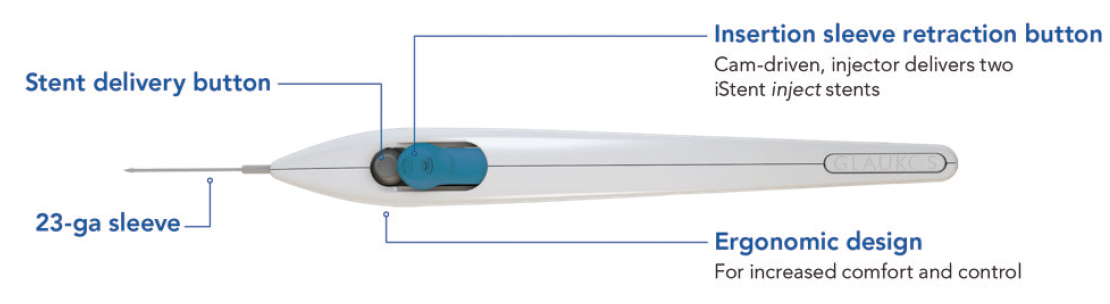
Figure 2. iStent inject delivery system.
Elegance and Symmetry
Both the iStent and iStent inject are elegant procedures, but iStent inject takes it to the next level by taking out some of the variability. Another advantage is that we know collector channels drain aqueous to the aqueous veins,2 so proximity to the aqueous veins is thought to increase flow through the stent. Having two stents with two patent openings increases the chance of being adjacent to an aqueous vein.
Due to the symmetrical stent design, there is no longer a right and a left stent. Surgeons no longer have to do a side-to-side movement or forehand or backhand. With iStent inject, surgeons approach the TM in a perpendicular motion, place the trocar through the center of the TM ensuring it is not biased one way or the other, and deploy the stent. Visualization remains extremely important, so I continue to encourage other surgeons to perfect their gonioscopy skills.
Two is Better Than One
Studies have demonstrated that implanting more than one stent can significantly increase the facility of outflow, thus leading to increased efficacy.2 As an example, laboratory studies conducted by the Mayo clinic have shown outflow facility after one iStent inject stent to increase from 0.16 to 0.38 µL/min/mm. After a second stent was implanted, outflow facility further increased to 0.78 µL/min/mm, representing a five-fold increase in outflow facility from baseline. An in-vivo human study conducted by Huang et al demonstrated when placed 2 to 3 clock hours apart, iStent inject provided immediate and more expansive flow post implantation, in addition to arcs of flow spanning 5 to 6 clock hours (Figure 3).
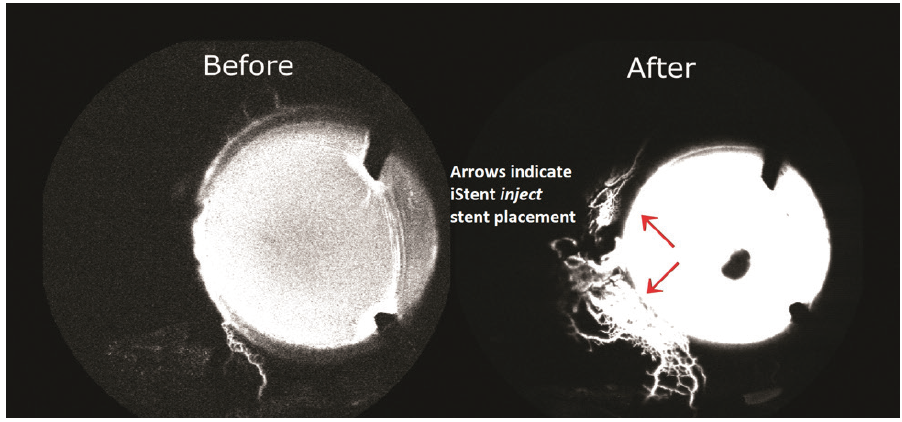
Figure 3. iStent inject demonstrated immediate and more expansive flow post implantation, arcs of flow that can span 5 to 6 clock hours, and the potential to reestablish flow in previously dormant outflow channels.
With iStent inject, I believe the first stent performs approximately 70% of the work while the second stent performs the rest. In the future, the possibility of adding a third stent is something that may unlock even further potential. There is still evolving science but consensus among the ophthalmic community is that multiple stents do provide additional improvement to outflow and increased efficacy.3
iStent inject Early Experience
The clinical benefits of the two patent openings was further confirmed in our own data presented at the 2019 ASCRS annual meeting. We looked at our first 39 consecutive iStent inject patients and found that we lowered IOP from 18.6 to 13.1 mm Hg at the 6-month mark and cut medications from 1.6 to 0.8 medications (Figure 4).
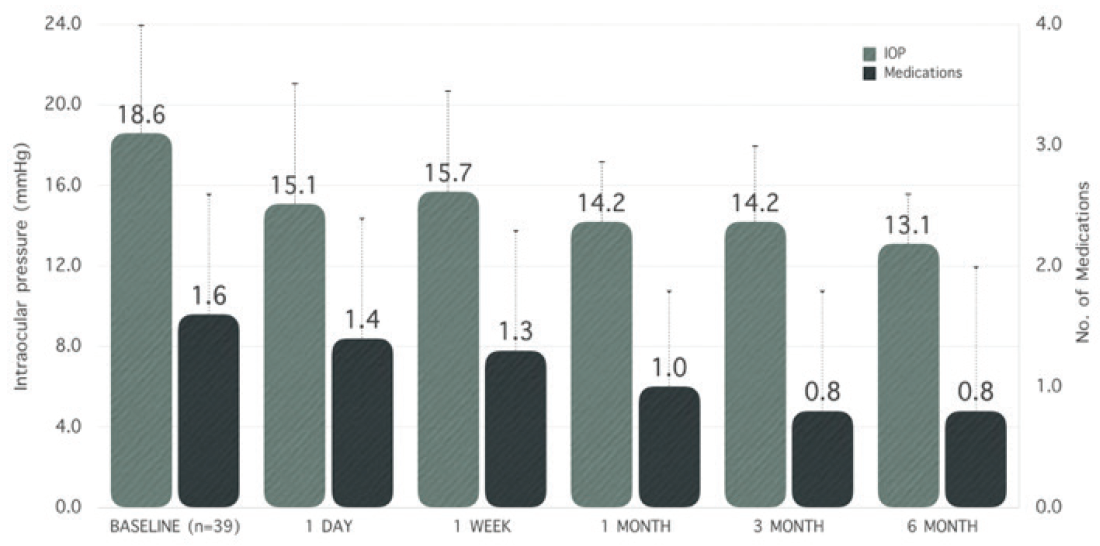
Figure 4. iStent inject IOP and medication reduction.
We also observed that 100% of our patients had an IOP of less than 18 mm Hg at the 6-month mark, and 83% had an IOP of less than 15 mm Hg. Theoretically, these strong results occurred because you have a larger drainage system with two stents that are accessing different downstream flow channels allowing a parallel circuit to be created that has less resistance to outflow (Figure 5).
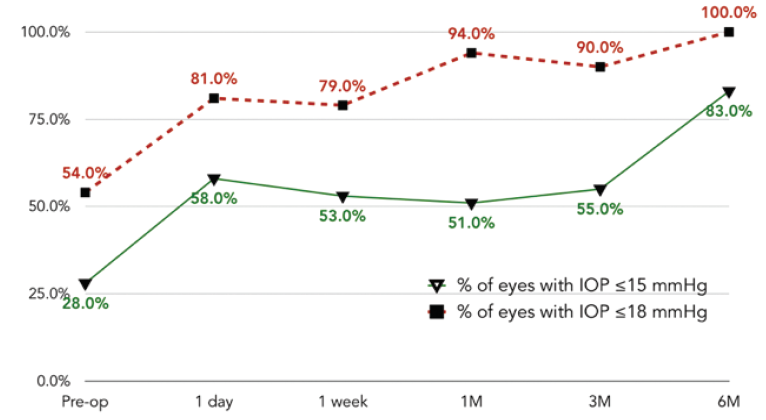
Figure 5. Proportional analyses: IOP ≤ 15 mm Hg and IOP ≤ 18 mm Hg.
Advantages of iStent inject Over iStent
The base difference, and demonstrated advantage, is that you get two stents with the iStent inject. This allows better flow through the trabecular system and the episcleral venous system, which indicates it lowers IOP better. Our early experience has confirmed the strong clinical performance that iStent inject can provide. The other advantage is the technical nature of the surgery. The iStent inject is more uniform in its design and removes some of the manual variables, allowing the procedure to be more precise and repeatable.
Both devices have a learning curve for new surgeons primarily around the visualization and delicate nature of the procedure. Both are imminently learnable by cataract surgeons. My experience has been that surgeons with previous experience with the first-generation iStent are comfortable transitioning to the second generation iStent inject, while those who are just getting started with the iStent inject vastly prefer it.
1. Le K, Saheb H. iStent trabecular micro-bypass stent for open-angle glaucoma. Clin Ophthalmol. 2014; 8:1937-1945.
2. Bahler C.K, Hann C.R, Fjield T, et al. Second-generation trabecular meshwork bypass stent (iStent inject) increases outflow facility in cultured human anterior segments. Am J Ophthalmol. 2012;153(6),1206-1213.
3. Manasses DT, Au L. The new era of glaucoma micro-stent surgery. Ophthalmol Ther. 2016;5(2):135-146.