


I was on the edge of Dana Point, California, when the excitement began to take hold; finally, a microinvasive glaucoma surgery (MIGS) residents course had come to fruition! Over the past decade, a glaucoma surgery revolution resulted in the rapid advent of surgical interventions targeting patients who are not best best served by current treatment modalities. MIGS aimed to fill the unmet need between medication/laser treatment and trabeculectomy/tube shunt surgery. Among residents, the MIGS space was leading to renewed interest in glaucoma fellowships,1 and there was growing debate concerning the inclusion of MIGS in residency training.2 Like all (if any) ophthalmology residents, I was staying up at night thinking about MIGS simulation for residency training3 and wondering why the MIGS industry had yet to create a formal resident course—until now.
the RESIDENT COURSE
In March 2017, I was fortunate to attend the inaugural MIGS residents course in Orange County, California, the Silicon Valley of the ophthalmic industry. This 1-day intensive-course, sponsored by Glaukos, featured morning education sessions and afternoon hands-on training co-chaired by John Berdahl, MD, and Thomas Samuelson, MD.

The most enjoyable part of this course for me was the enthusiasm of the participants, hands down. To engage this audience at the very end of their residency, optimistic and energetic, was a delight.
—Thomas Samuelson, MD
Education session. The organizers and speakers discussed surgical options that included a comprehensive review of all the device companies in the MIGS space. The education session covered the various approaches in the MIGS spectrum (trabecular, suprachoroidal, and subconjunctival) in a uniquely device-agnostic fashion.
Dr. Samuelson started the morning with an overview of glaucoma surgery and a discussion on the rationale for MIGS as an individualized therapeutic approach. This was followed by a review of how to address combined cataract and glaucoma surgery. There are few teachers who can take students through the history of surgical evolution as a storyteller and an innovator. Dr. Samuelson’s examination of the past enabled us to viscerally experience the necessary trials and tribulations of filtration surgery in taking on the high risk for the benefit of saving vision in advanced glaucoma. After, we followed his path of innovation that established MIGS as an approach for mild to moderate glaucoma.
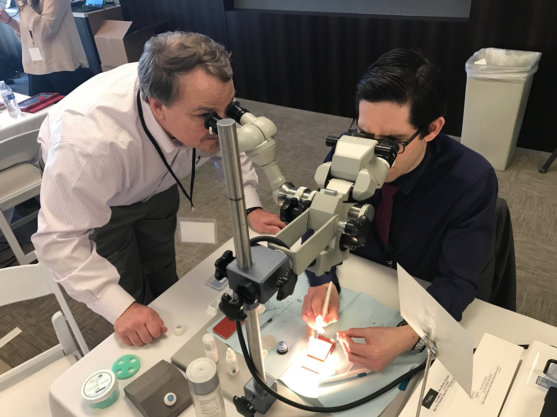
Figure 1 | In the training lab, each resident had his or her own microscope station and surgical instruments.
Next, Dr. Berdahl delivered a discussion on the critical elements of the MIGS technique, focusing on the importance of gonioscopy and visualization, with many example images and videos, as well as pearls and pitfalls for practice. Following, he systematically reviewed the ocular target areas for MIGS approaches: the trabecular meshwork/Schlemm canal, supraciliary/suprachoroidal space, and subconjunctival space. Then Dr. Berdahl presented surgical videos from his personal archives of nearly every commercial and experimental MIGS device and procedure. Notably, he showed not just the pristine surgical scenarios but also cases that spanned the complexity spectrum. He discussed how he and his fellows navigated difficult and unexpected situations. It was these moments that gave the audience an appreciation for the mindset and surgical skills required to adopt MIGS.

The course covered all of the currently available MIGS interventions, and it was delightful to see the enthusiasm and engaged learners.
—John Berdahl, MD
Dr. Samuelson and Dr. Berdahl did not serve as mere surgical instructors but as seasoned philosophers of glaucoma care, imparting wisdom to a new generation of young surgeons eager to provide the best care possible. Glaucoma is a lifelong chronic disease that can be managed, and, as the treatment perspective shifts to viewing glaucoma as a surgical disease, we are lucky to have such mentors pushing and inspiring us to do better for our patients.
Hands-on training. After the didactic sessions, the resident physicians were eager to get hands-on practice. We were transported to the Glaukos headquarters and got a tour of the facilities before stepping into the training lab. While the farm-to-table analogy may seem like a stretch, it was fascinating to meet the people involved with the world’s smallest medical implant from production and quality assurance, until its arrival at the operating room, ready for implantation.
Time constraints are the most significant limitation to the course. There is too much material to cover each topic in adequate detail. In addition, while the wet lab is excellent, nothing duplicates real surgery in living human tissue. It would be enjoyable to work with the residents in their own operating rooms as they do their first cases utilizing the skills transferred during the course.
—Thomas Samuelson, MD
In the training lab, each resident had his or her own microscope station and surgical instruments. The Glaukos engineering team created unique non-biologic 3D printed models with tactile feedback that allowed for repeated and deliberate practice of the MIGS skills required for successful device insertion. Uniquely, we had the opportunity to work with the commercial iStent product as well as the iStent Inject and iStent Supra investigational devices (Glaukos). After several hours of focused practice, we boarded the shuttle back to the hotel for dinner.

Figure 2 | Attendees received a wooden cigar-style box containing an iPrism surgical gonioscopic lens and iPrism Clip view stabilizer (Glaukos).
SMOOTHING THE TRANSITION
As the sun was setting over the Pacific Ocean, we had dinner with the organizers and faculty before a final farewell. All residents were provided with a combination of parting gifts so that we could build on our excitement and continue our MIGS education: a copy of Minimally Invasive Glaucoma Surgery: A Practical Guide4 and a wooden cigar-style box containing an iPrism surgical gonioscopic lens and iPrism Clip view stabilizer (Glaukos; Figure 2).
Overall, the inaugural MIGS resident course was a huge success. If I forced myself to consider how this course could have been better, I wish it had been longer and had a wet lab component that used animal eyes or a model system that simulated the dynamics of a biological intraocular surgical environment. MIGS has revolutionized the landscape of glaucoma management. Resident physicians would be well served to attend this course to smooth the transition of skills transfer and implementation.
1. Brown R, Boyle E. Interest growing for glaucoma fellowships. EyeWorld. 2013. Available at: https://www.eyeworld.org/article-interest-growing-for-glaucoma. Accessed April 25, 2017.
2. Khouri AS, Vold SD. Point/counterpoint: should MIGS be included during residency training? Glaucoma Today. 2015. Available at: https://glaucomatoday.com/2015/06/pointcounterpoint-should-migs-be-included-during-residency-training/. Accessed April 25, 2017.
3. Bussel II. MIGS simulation. Glaucoma Today. 2017. Available at: https://glaucomatoday.com/2017/02/migs-simulation/. Accessed April 25, 2017.
4. Realini T. Review of minimally invasive glaucoma surgery: a practical guide. EyeWorld. 2017. Available at: https://www.eyeworld.org/review-minimally-invasive-glaucoma-surgery-practical-guide. Accessed April 30, 2017.

