


A 35-year-old man initially presented to the emergency room with an open-globe injury in his right eye from a knife laceration. At the time of injury, he had a visual acuity of counting fingers at 1 foot, no relative afferent pupillary defect, and a corneal laceration with anterior lens capsule rupture. His subsequent treatment course was extensive, consisting of an open right globe repair, pars plana vitrectomy with total lensectomy, and placement of a secondary scleral-sutured IOL over 10 months. His visual acuity improved to 20/60 without correction.
Two months later, the patient presented with new symptoms of photophobia, foreign body sensation, and worsening vision in his right eye (20/70). His intraocular pressure (IOP) was 21 mm Hg. Anterior segment exam was significant for an iris cyst at 8 o’clock, posterior to the corneal laceration and consistent with an epithelial downgrowth implantation cyst (Figure 1). Due to the small size, the cyst was observed. However, the cyst continued the grow on subsequent exams, covering 33% of the anterior chamber from 5:30 to 9 o’clock and partially displacing the IOL posteriorly (Figure 2).
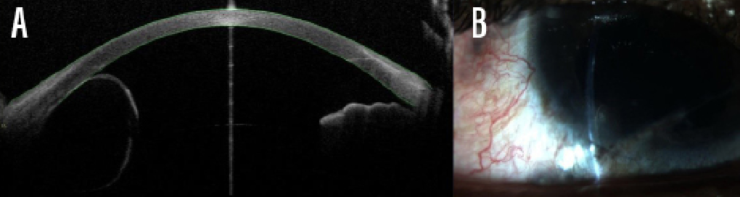
Figure 1 | Images of an iris cyst at 8 o’clock 1 year after penetrating injury and 2 months after scleral-sutured IOL on anterior segment optical coherence tomography (A) and at the slit lamp (B).
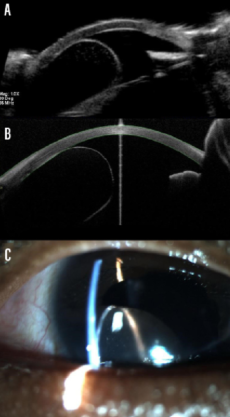
Figure 2 | Images of an iris cyst covering 33% of the anterior chamber 2 months after initial presentation on ultrasound biomicroscopy (A), on anterior segment optical coherence tomography (B), and at the slit lamp (C).
The decision was made to aspirate the cyst in the operating room, as described by Behrouzi et al.1 A 30-gauge needle was inserted 2 mm behind the limbus into the cyst to deflate the cavity completely. A triple stopcock was used to inject 98% ethanol into the cyst so that the needle did not need removal. After 2 minutes of ethanol treatment, the iris cyst was again completely deflated (Video). Postoperative day 1 was complicated by a high IOP of 44 mm Hg, which resolved with an in-office paracentesis and acetazolamide 500 mg tablets twice a day. At the slit lamp, cyst remnants were observed between 6 and 7 o’clock (Figure 3).
Video | Ethanol treatment of an iris epithelial inclusion cyst.

Figure 3. Slit-lamp image of an iris cyst 1 day after ethanol irrigation.
Four weeks post-procedure, following a topical steroid taper course similar to that after cataract surgery, the patient’s uncorrected vision returned to 20/60, and his IOP was stable on brimonidine and timolol (»Combigan; Allergan) twice a day. The residual cyst was observed at 6 to 8 o’clock on slit-lamp exam and remains stable in size. Given the relative simplicity of the procedure, we plan to repeat aspiration and ethanol injection if the cyst regrows.
DISCUSSION
Our patient presented with an iris cyst within a year of his penetrating injury. Given the mechanism of injury and location of the cyst, the clinical diagnosis of an epithelial inclusion cyst (EIC) secondary to traumatic epithelial downgrowth was made. A growing cyst can cause corneal decompensation, loss of vision, and closed-angle glaucoma if not treated.2
In the literature, numerous treatment options are evaluated for EIC, including laser photocoagulation, endodiathermy, intracameral antimetabolite injections, and, the most invasive, surgical resection; however, no method has been proven to be superior.2-9 Resection can cure the cyst but causes significant ocular morbidity, as the adjacent structures must be removed.10 Also, if the cyst ruptures during removal, there will be diffuse epithelial downgrowth within the anterior chamber—a catastrophic complication that often results in loss of the eye.
Our patient had undergone multiple reconstructive eye surgeries, so we chose the least invasive method to minimize further morbidity. Subsequent treatments may be needed if not all of the cyst epithelial cells were destroyed by the first application, but this method is generally easy to perform and results in minimal postoperative complications.1,11
SUMMARY
Iris EIC secondary to surgery or penetrating trauma can be a difficult problem to solve. Although there are many treatment options, the ethanol infusion technique is one of the safest ways to involute a single-cavity iris EIC. Our case and accompanying video above highlight the relative safety and ease of this technique in treating a post-traumatic iris EIC.
1. Behrouzi Z, Khodadoust A. Epithelial iris cyst treatment with intracystic ethanol irrigation. Ophthalmology. 2003;110:1601-1605.
2. Lai MM, Haller JA. Resolution of epithelial ingrowth in a patient treated with 5-fluorouracil. Am J Ophthalmol. 2002;133:562-564.
3. Gupta V, Rao A, Sinha A, Kumar N, Sihota R. Post-traumatic inclusion cysts of the iris: a longterm prospective case series. Acta Ophthalmol Scand. 2007;85:893-896.
4. Maumenee AE, Paton D, Morse PH, Butner R. Review of 40 histologically proven cases of epithelial downgrowth following cataract extraction and suggested surgical management. Am J Ophthalmol. 1970;69:598-603.
5. Naumann GO, Rummelt V. Block excision of cystic and diffuse epithelial ingrowth of the anterior chamber. Report on 32 consecutive patients. Arch Ophthalmol. 1992;110:223-227.
6. Scholz RT, Kelley JS. Argon laser photocoagulation treatment of iris cysts following penetrating keratoplasty. Arch Ophthalmol. 1982;100:926-927.
7. Tomlins PJ, Savant V, Quinlan M. Failure of intracameral fluorouracil to resolve an epithelial ingrowth following clear corneal cataract surgery. J Cataract Refract Surg. 2007;33:923-924.
8. Tsai JC, Arrindell EL, O’Day DM. Needle aspiration and endodiathermy treatment of epithelial inclusion cyst of the iris. Am J Ophthalmol. 2001;131:263-265.
9. Yu CS, Chiu SI, Tse RK. Treatment of cystic epithelial downgrowth with intralesional administration of mitomycin C. Cornea. 2005;24:884-886.
10. Haller JA, Stark WJ, Azab A, Thomsen RW, Gottsch JD. Surgical management of anterior chamber epithelial cysts. Am J Ophthalmol. 2003;135:309-313.
11. Shields CL, Arepalli S, Lally EB, Lally SE, Shields JA. Iris stromal cyst management with absolute alcohol-induced sclerosis in 16 patients. JAMA Ophthalmol. 2014;132:703-708.

