


Since their introduction more than 2 decades ago,1-2 capsular tension rings (CTRs) have evolved into an important tool for the management of cataract surgery in the setting of zonular weakness. After insertion, CTRs generate a centrifugal force on the equator of the capsular bag, equally distributing forces and transmitting tension from normal zonules to affected areas.
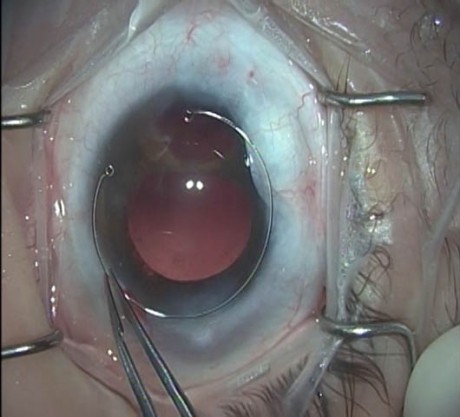
Figure 1. A standard CTR.
TYPES
Different types of CTRs are available for different settings. A standard CTR (Figure 1) is a PMMA, ring-shaped device with one eyelet at each end. A modified Cionni CTR3 (Morcher; Figure 2) has the same configuration but with one or two additional eyelets for scleral fixation, depending on the model. The Ahmed capsular tension segment4 ([CTS] Morcher; Figure 3), a modification of the original Cionni ring, is smaller in size and covers around 120º of capsular bag circumference.
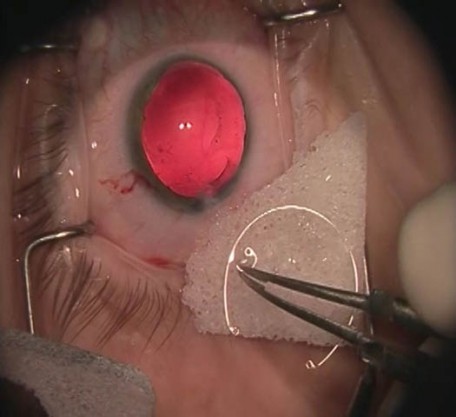
Figure 2. A Cionni modified CTR.
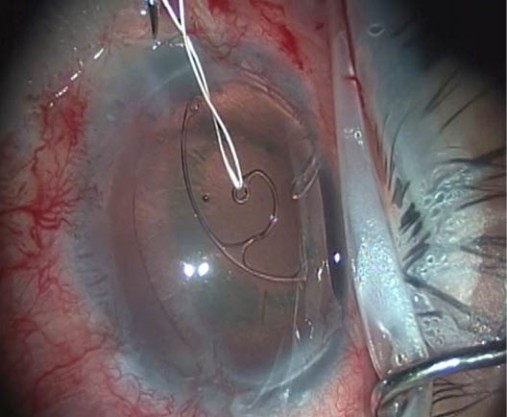
Figure 3. A capsular tension segment.
INDICATIONS
These devices should be considered in every case of evident or suspected zonular deficiency and ideally should be available in every operating room.
In general, when less than 3 clock hours of zonules are compromised, a standard CTR is sufficient to ensure bag stability. Over that range, or if it is felt that a standard ring will not provide enough bag stability, scleral fixation of the CTR is recommended. If scleral-fixated rings are not available or if the surgeon is not comfortable with the surgical technique, a standard CTR can be implanted and then repositioned 1 month postoperatively when bag fibrosis has occurred.
CTRs should not be implanted if a posterior capsular rupture has or might have occurred; in this setting, CTSs should be favored.
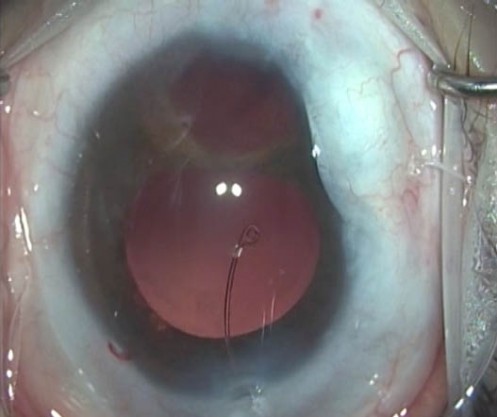
Figure 4. Manual insertion of a CTR.
SURGICAL TECHNIQUE
CTR insertion can be achieved either manually (Figure 4) or by an injector, based on surgeon preference. In our opinion, manual insertion provides additional bag resistance feedback, which allows us to modify the insertion process accordingly.
Nontoothed forceps are used to hold the CTR and gently dial it into the capsular bag through the main wound, directed under the anterior capsule. Resistance during insertion, which is normally created by trapping a capsular fold with the leading eyelet of the ring during insertion and made evident by capsular striae formation, can be dealt with by gently backing up with the ring and then resuming the insertion.
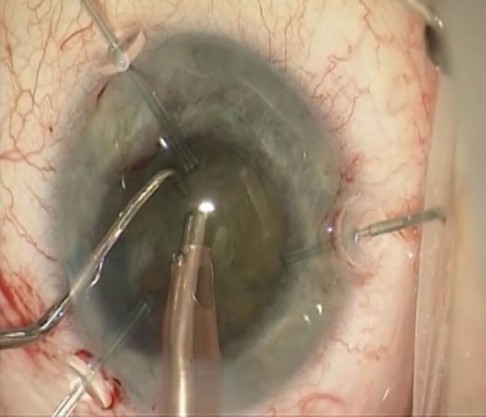
Figure 5. Capsular retractors.
Timing of CTR insertion will vary based on the surgical circumstances, but ideally a CTR should be inserted after the cataract and cortex have been removed and prior to insertion of the IOL. If the zonular weakness does not allow for proper phacoemulsification or cortex removal, the capsular bag can be stabilized with capsular retractors (Figure 5) or with one or more CTS, avoiding premature insertion of the CTR.
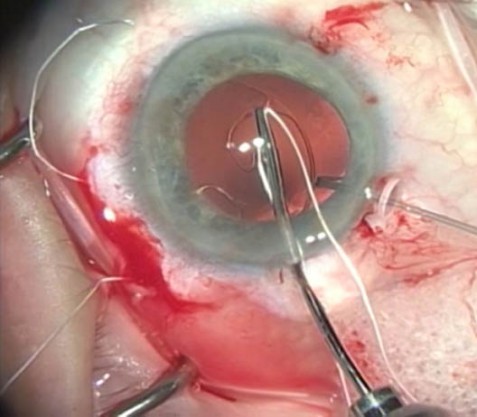
Figure 6. Insertion of a CTS with a prethreaded ePTFE suture through the fixation eyelet.
For scleral fixation, although this is an off-label use, we strongly favor expanded polytetrafluoroethylene5 ([ePTFE] Gore-Tex; W.L. Gore & Associates) over polypropylene sutures, mainly due to the limited lifespan of polypropylene and the need for long-term fixation. We use the ePTFE suture to prethread a Cionni modified CTR, one or more CTS (Figure 6), or a combination through the fixation eyelet; we insert the selected device into the capsular bag, making sure the fixation eyelet is above the anterior capsule.
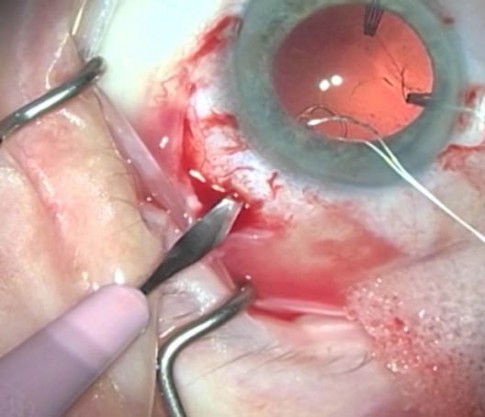
Figure 7. Sclerotomy created with a 15° blade at the sulcus level.
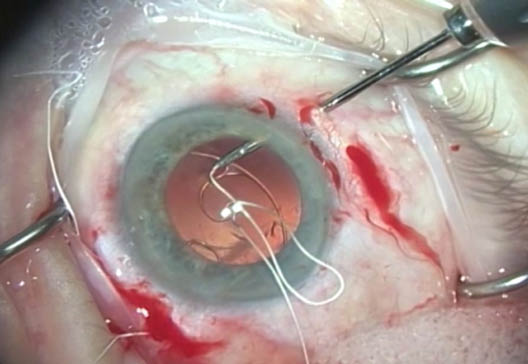
Figure 8. ePTFE suture retrieval with 25-gauge microforceps through a ciliary sulcus level sclerotomy.
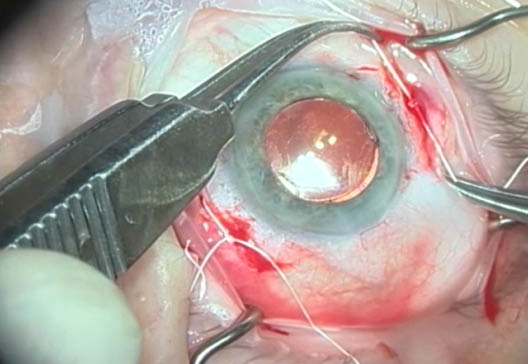
Figure 9. ePTFE tension adjustment based on bag centration and Purkinje reflexes.
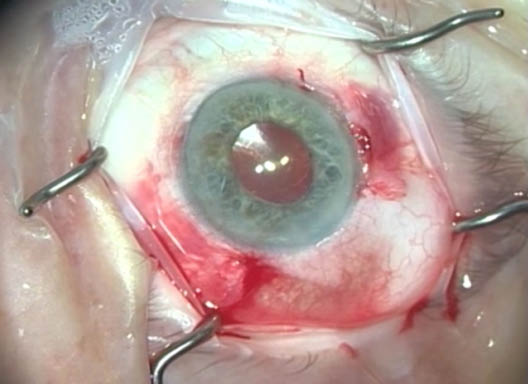
Figure 10. Final result with a centered capsular bag fixated to the scleral wall. Both knots are buried into the scleral wall, and sutures are covered by conjuctiva.
Next, we create two sclerotomies with a 15º blade (Figure 7), 2 mm apart, at the sulcus level, in order to retrieve both ends of the ePTFE suture using 23- or 25-gauge microforceps (Figure 8). We then tie the knots with the necessary tension for proper centration based on the Purkinje reflexes (Figure 9), which will result in a centered and stable bag fixated to the wall of the eye. The knots must be rotated into the scleral wall and the sutures covered by conjunctiva (Figure 10).
COMPLICATIONS
The most feared complication while inserting a CTR is breaking the posterior capsule during the insertion. This can be prevented by avoiding any resistance spots, which basically indicate that the leading edge of the ring has caught a capsular fold on this floppy bag and that, if further pressure is applied, the leading edge will go through the bag unless the ring is partially retrieved and redirected.
The same mechanism can explain another potential complication, which is iatrogenic zonular damage during insertion. In both cases, the key is to avoid fighting capsular bag resistance and to modify the direction of insertion. Further, inserting the ring toward the area of weakness instead of opposite to it will decrease the likelihood of further zonular damage.
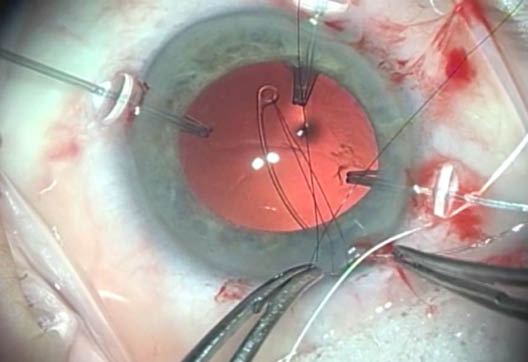
Figure 11. 10-0 nylon through the leading eyelet of a CTR, allowing for a countertraction with a second instrument through the main wound.
Our preferred technique for avoiding these two unfortunate scenarios is to prethread the leading eyelet of the CTR with a 10-0 nylon suture.7 This enables countertraction to be applied with microforceps during insertion (Figure 11), either from the main wound or from a paracentesis, depending on the location of entrapment and the direction we would like the ring to bend toward. This suture is later cut and gently removed when the insertion process is completed. Newer-generation CTRs, such as the Morcher CTR type 13 series, are designed with a bent leading eyelet to decrease the likelihood of these complications and reduce the risk of entrapment; some feature a blue tint for better visualization.
Another complication associated with CTR use is inadvertent insertion of the ring into the ciliary sulcus. To deal with this complication, we first must be able to recognize it; therefore, slow and gentle insertion of the ring is recommended. Trypan blue can be used to stain the anterior capsule in early cases in order to prevent this unfortunate scenario. This step will aid in visualizing the exact location of the leading edge of the ring during insertion and of the trailing edge before it is finally released into the bag.
Second, a flattening effect should be seen on the bag after CTR insertion. The absence of any effect on the floppiness of the bag or at least partial centration of a subluxed bag are signs of a potential suboptimal insertion. A malpositioned ring should ideally be retrieved and reinserted. The iris should be displaced to the periphery in order to aid with visualization, and a Sinskey hook can be used to dial the leading edge of the ring first out of the ciliary sulcus and then, using a second instrument, to the main wound, where it can be retrieved to attempt a second insertion.
PEARLS
We recommend using a CTR in every case of pseudoexfoliation, even if the zonular apparatus seems stable. Pseudoexfoliation is a progressive condition, and even though the ring will not prevent future subluxation, it will considerably decrease the complexity of repositioning the capsular bag if it becomes necessary.
Different ring diameters are available. Make sure to measure the white-to-white in unusually sized eyes before selecting the desired CTR.
In small eyes, such as those with nanophthalmos or in children with zonular weakness, even the smaller rings can be too big. One alternative is to manually bend the ring before insertion in order to reduce the external diameter of the CTR, which will not only allow for the ring to fit in this smaller bag but will also significantly aid in its insertion.
If a CTR is going to be inserted in a bag that already holds a posterior chamber IOL, we recommend performing the insertion counterclockwise to avoid entrapment of the CTR at the edge of the haptic.
CONCLUSION
CTRs are an important tool in every anterior segment surgeon’s armamentarium; therefore, it is advisable to become confident in their manipulation. Proper CTR use can aid in the management of zonular weakness and complex cataract surgery, both by reducing intraoperative stress and the need for secondary procedures for bag recentration.
1. Hara T, Yamada H. Equator ring for the maintenance of the completely circular contour of the capsular bag equator after cataract removal. Ophthal Surg. 1991;22:358.
2. Leger U, Witschel BM, Lim SJ, et al. The capsular tension ring: a new device for complicated cataract surgery. Paper presented at: the Third American-International Congress on Cataract, Intraocular Lenses, and Refractive Surgery; May 11, 1993; Seattle, Washington.
3. Cionni RJ, Osher RH. Management of profound zonular dialysis or weakness with a new endocapsular ring designed for scleral fixation. J Cataract Refract Surg. 1998;24:1299-1306.
4. Ahmed IK, Kranemann C, Crandall AS. Capsular hemi-ring: next step in effective management of profound zonular dialysis. Film presented at: the ASCRS Film Festival; April 2003; San Francisco, California.
5. Snyder ME, Perez MA. Dislocation of intraocular lenses. In: Roy FH, Tindall R, eds. Master Techniques in Ophthalmic Surgery. 2nd ed. JP Medical Publishers; 2015: 697-704.
6. Price MO, Price FW Jr, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 2005;31:1320-1326.
7. Perez MA, Snyder ME. Strategies to manage zonular deficiency. Cataract & Refractive Surgery Today Europe. February 2015:1-5