
THE CASE
A 65-year-old woman presented to our clinic with significant redness, pain, and blurry vision in her right eye (OD). She reported ocular-involving Stevens-Johnson syndrome (SJS) after taking allopurinol 3 years prior. Past surgeries included bilateral tarsorrhaphy as well as pars plana vitrectomy/lensectomy and sulcus IOL placement OD. She was using cyclosporine 0.05%, besifloxacin 0.6%, and difluprednate 0.05% drops as well as acetaminophen-codeine.
The patient’s visual acuity was 20/400 OD, with no improvement on pinhole refraction. Slit-lamp examination of the right eye revealed conjunctival injection and a persistent corneal epithelial defect with scattered scars.
Due to her history of SJS, the persistent epithelial defect, and constant redness and pain, she underwent buccal mucous membrane grafting to the limbus, with accompanying amniotic membrane transplantation to the ocular surface 1 month later. Photographs of her right eye during the postoperative course are shown in Figure 1.
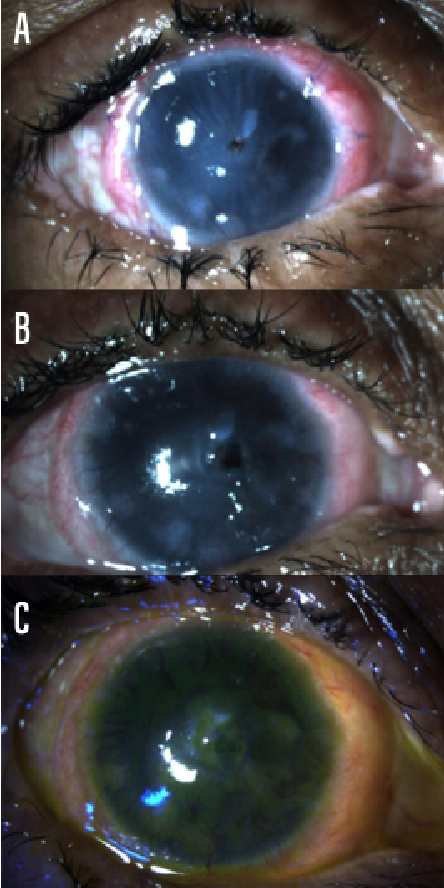
Figure 1 | Postoperative photographs of the patient’s right eye at 3 weeks (A), 11 weeks (B), and 17 weeks (C) postoperatively.
Three weeks postoperatively, the patient reported no pain in her right eye. The buccal mucosal graft was integrating well 360° perilimbally, and the amniotic membrane was visible overlying the cornea (Figure 1A). However, there was a Seidel-negative area of central corneal thinning; 2-octyl cyanoacrylate (Dermabond; Ethicon) adhesive was placed to cover the thin area, and trimethoprim/polymyxin B was prescribed.
At 11 weeks postoperatively, the patient reported aching pain in the right eye and was found to have a new epithelial breakdown (Figure 1B). She received an additional amniotic membrane graft, which was successful. Six weeks after placement of the second graft, fluorescein staining revealed no persistent epithelial defects, and the buccal mucosa graft was in place with minimal ocular surface inflammation (Figure 1C). She was scheduled for penetrating keratoplasty (PKP) to restore visual acuity.
DISCUSSION
SJS can cause devastating chronic ocular surface inflammation and limbal stem cell deficiency.1 In these cases, interventions such as PKP and keratolimbal allografts are not ideal for several reasons.2,3 First, PKP and keratolimbal allografts are antigenic because they are allogeneic. Second, the ocular surface is composed of both the cornea and conjunctiva, but these grafts address only corneal problems.
On the other hand, direct buccal mucosa grafts at the limbus are autologous and can replenish both the corneal and conjunctival surfaces.4 Additionally, buccal mucosal epithelium is similar histologically to conjunctival and corneal epithelia.5 Oral mucosal tissues are also readily harvested, and donor sites heal quickly. For these reasons and others, buccal mucosa grafts are already used to treat symblepharon and lid margin pathology in chronic ocular-involving SJS.6
The buccal mucosal graft immediately relieved our patient’s pain and conjunctival redness and, after two additional amniotic membrane grafts, eventually helped relieve her corneal epithelial defect. This case illustrates that buccal mucosal transplantation is a reasonable and simple, albeit not perfect, solution to a very challenging problem.
Supported in part by the Hermann Eye Fund.
1. Kohanim S, Palioura S, Saeed HN, et al. Acute and chronic ophthalmic involvement in Stevens-Johnson syndrome/toxic epidermal necrolysis – a comprehensive review and guide to therapy. II. Ophthalmic disease. Ocul Surf. 2016;14(2):168-188.
2. Sotozono C, Ueta M, Koizumi N, et al. Diagnosis and treatment of Stevens-Johnson syndrome and toxic epidermal necrolysis with ocular complications. Ophthalmology. 2009;116(4):685-690.
3. Liang L, Sheha H, Tseng SCG. Long-term outcomes of keratolimbal allograft for total limbal stem cell deficiency using combined immunosuppressive agents and correction of ocular surface deficits. Arch Ophthalmol. 2009;127(11):1428-1434.
4. Liu J, Sheha H, Fu Y, Giegengack M, Tseng SC. Oral mucosal graft with amniotic membrane transplantation for total limbal stem cell deficiency. Am J Ophthalmol. 2011;152(5):739-747.
5. Nakamura, Takahiro. Non-ocular sources for cell-based ocular surface reconstruction. In: Holland EJ, Mannis MJ, Lee WB, eds. Ocular Surface Disease: Cornea, Conjunctiva, and Tear Film. Philadelphia, PA: Elsevier-Saunders; 2013; 373-383.
6. Henderson H, Collin J. Mucous membrane grafting Dev Ophthalmol. 2008;41:230.

