


The best things in life may be free, but the best instruments purchased in your first few years of practice are priceless. These are the tools that will help sharpen your surgical skills, affect your outcomes, and play a pivotal role in building your reputation as an ophthalmic surgeon. When you look at it from that perspective, it’s easy to see how the return on investment from these early purchases transcends dollars and cents.
I am a cornea and refractive surgery specialist heading into my fourth year out of fellowship, and I recently started a new position with Acuity Eye Group. My initial purchases reflect my focus on refractive cataract surgery, with an aim toward growing the refractive portion of my practice, and my increasing involvement in microinvasive glaucoma surgery (MIGS). These tools are the perfect complement to my present position and will likely be essential to any ophthalmic surgery endeavor that I pursue in the future.
DAVIS MD ONESTEP PREOPERATIVE MARKER
The Davis MD OneStep preoperative marker (Mastel; Figure 1) tops the list of the best purchases I’ve made so far. This instrument is easy to use, precise, and efficient; it actually eliminates several steps during surgery, making my toric IOL cases almost as fast as my non-toric IOL cases. The rotating head of the marker is laser engraved in 5° increments for marking the steep meridian; I can dial it to the exact degree that I am trying to place my toric lens.

Figure 1 | The Davis MD OneStep preoperative marker is precise and efficient.
I mark the patient while he or she is sitting up. The gravity alignment head eliminates the need for controlling orientation, and the fins are sharpened and appropriately curved to impress/divide the epithelium without tearing. The marker’s metallic grooves leave linear indentations in the cornea that last for several hours. This is ideal because I don’t have to use a Mendez ring or an awkward half-moon instrument to make my toric marks. I simply use a fine-tip marker, and the ink bleeds into the indentation, giving me a very precise alignment. It is important to note that ink is not necessary; the dry marks create sharp epithelial demarcations.
OSHER/NICHAMIN FIXATION RING
The Osher/Nichamin Fixation Ring (Mastel) with the Jarvi Double pattern (Figure 2) is another of my earliest purchases, and it remains a go-to tool in my surgical armamentarium. This device helps ensure consistent, quality limbal relaxing incisions (LRIs) even without access to a femtosecond laser. The most important feature are its teeth. I simply place the fixation ring holding the eye in place, place my marks along the ring for my arcuate incision, and then use it as a guide to help stabilize the diamond blade. I use the lip of the ring to guide the scalpel footplates to make uniform arcuate incisions. With the pattern in view, I can make arcuate keratotomies (AKs) of the right length with minimal steps.

Figure 2 | The Osher/Nichamin Fixation Ring ensures LRI quality and consistency.
PHD II STEP DIAMOND BLADE
The PhD II Step Diamond Blade (Mastel; Figure 3) completes the trio of Mastel instruments that are key to my surgical technique. I purchased these products on my own, without assistance from my practice; while the cost was considerable, particularly for the diamond blade, it was worth every penny. This diamond blade is extremely precise. It has a full extension step for use as a freehand blade for paracentesis or wound extension, along with a 600-mm depth setting for LRIs and AKs. I typically set it at 600 mm and have had great success.

Figure 3 | The PhD II Step Diamond Blade has a 600-mm depth setting for LRIs and AKs.
I once used a different diamond blade and had a small corneal perforation in the case. One complication was all it took to reinforce my exclusive use of the PhD II Step Diamond Blade. I relied on this diamond knife for LRIs even more before I had access to a femtosecond laser. If you are a young surgeon headed to a practice where you will not have access to a femtosecond laser, you can feel confident about your surgical skills if you have a quality diamond blade such as this.
SEIBEL CAPSULORHEXIS FORCEPS
The 23-gauge Seibel Capsulorhexis Forceps (MicroSurgical Technology; Figure 4) are another instrument that I favor. These forceps have a 23-gauge shaft and enable extremely precise capsulorhexis creation. This instrument fits through a paracentesis as small as 1 mm. In main incisions, this feature provides significantly more room in the incision while minimizing viscoelastic egress. Another benefit is that these forceps enable me to see through the grasping tips, even in the closed position, which allows me to maintain visibility on the capsule throughout the entire capsulorhexis (Figure 5).
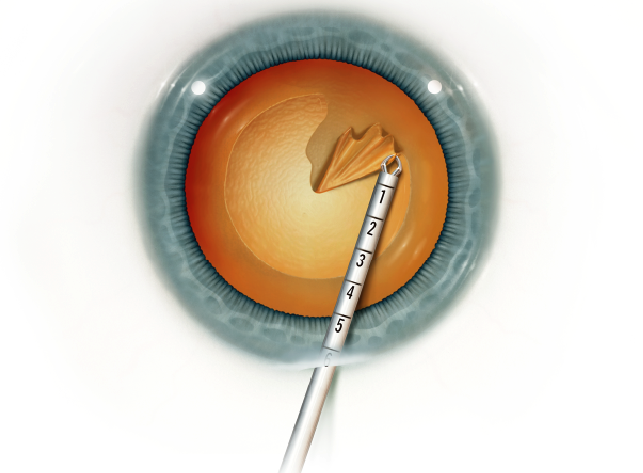
Figure 4 | The 23-gauge Seibel Capsulorhexis Forceps fit through a 1-mm paracentesis.
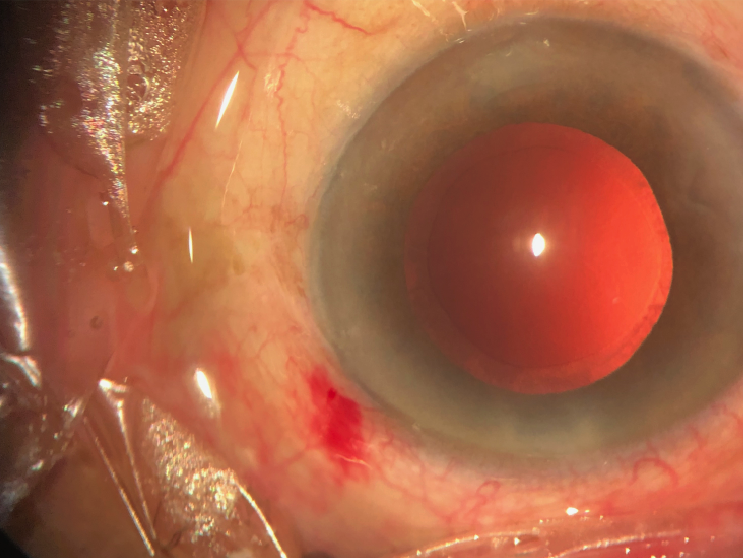
Figure 5 | A manual capsulorhexis made using the Seibel Capsulorhexis Forceps.
DUET BIMANUAL I/A
The Duet BiManual I/A System (MicroSurgical Technology; Figure 6) is another of my favored surgical implements. It fits through a standard 1-mm paracentesis, eliminating the need to move to a larger incision. This system minimizes the risk of capsular issues and allows for excellent wound stability. It gives me full access to all of the cortex, making removal of subincisional cortex easy. Additionally, my incidence of wound leakage is extremely low, and I believe that it is due, in large part, to my use of the smooth Duet handpiece for irrigation and aspiration, which gives my main incision plenty of time to seal and allows for excellent toric IOL stability.

Figure 6 | The Duet BiManual I/A System allows for excellent toric IOL stability.
BERDAHL GONIO PRISM STABILIZER
Another item that I am pleased I added to my armamentarium is the Berdahl Gonio Prism Stabilizer (Storz Ophthalmic Instruments;https://youtu.be/uj2Moi_8etw). This device is particularly useful given the increasing popularity of MIGS. When I started out, I used a gonioprism without a stabilizer. The eyes would move, the patients would move, and it was frustrating. The Berdahl stabilizer fits around the gonioprism and holds the eye in place, allowing for better control of the eye during MIGS procedures. My recommendation to novice surgeons is to ask the appropriate person at your practice to purchase this device.
CONCLUSION
The items described above have been instrumental to my maturation as an ophthalmic surgeon. If you are in the early stages of your career and feel overwhelmed by the array of instrument choices at your disposal, I recommend that you follow my lead. I have relied on these instruments for the past 3 years and can attest to their benefits and overall worth.
