


More and more, we are seeing patients request complete spectacle independence, and of equal frequency is the demand for intermediate vision. With the digital world evolving, patients now desire the ability to see their mobile devices at arm’s length as well as close up.
A few years ago, we decided to introduce a new trifocal presbyopia-correcting IOL into our practice, as patients were coming back mostly happy with their multifocal IOLs but still reporting a compromise in quality of vision, mainly at intermediate distance, as well as dysphotopsia phenomena. We discussed looking at a mix-and-match lens approach but ultimately determined that giving patients a larger range of vision with the AT LISA trifocal IOLs (Carl Zeiss Meditec) was a better option. We started implanting these lenses in 2012 and have implanted 250 so far, including 25 of the toric version.
IOL Specifications
The AT LISA tri 839MP is a one-piece diffractive aspheric IOL made of a hydrophilic acrylic material with hydrophobic surface properties. It has an optic diameter of 6.0 mm and a total diameter of 11.0 mm.
The AT LISA tri 839MP has a +3.33 D near add (equivalent to 40 cm) and a +1.66 D intermediate add (equivalent to 80 cm). The lens comes preloaded in a diopter range of 0.00 D to +32.00 D. The toric version, the AT LISA tri toric 939MP, is available in a range of powers for sphere (-10.00 D to +32.00 D) and cylinder (1.00 D to 12.00 D).
Designed for microincision cataract surgery, the AT LISA tri 839MP can be implanted through a 1.8-mm incision. The lens has an 87% mean light transmission, which is higher than most multifocal IOLs, and the light distribution is 50% to distance, 20% to intermediate, and 30% to near.
The AT LISA tri 839MP.
Patient Selection and Clinical Pearls
Patient selection is considered to be the most important factor in the implantation of all types of multifocal IOLs. A compromise in quality of vision, especially under dim light conditions, is still part of the game.
In our trifocal IOL patients, we have seen a reduction in glare and halos at night compared with other multifocal lenses. Regardless, it is still part of our consent process to inform patients of these potential side effects, and frequent night drivers would not be considered ideal candidates. A good potential visual acuity in both eyes and stereopsis without other pending ocular pathologies are needed to achieve good results.
Similar to other multifocal IOLs, with AT LISA tri implantation, it is essential to achieve emmetropia without significant astigmatism and to manage the corneal surface in a sufficient way; therefore, we choose to implant the AT LISA tri toric even for low grades of astigmatism.
So far, we are very satisfied with the accuracy of our postoperative refractions, and our enhancement rate has been exceedingly low (around 5%). However, the option to perform refractive enhancements is still valuable and necessary in some cases.
In our experience, patients implanted with the AT LISA tri 839MP have achieved high spectacle independence for near, intermediate, and distance. Readers are usually only required for fine print or reading in dim light conditions.
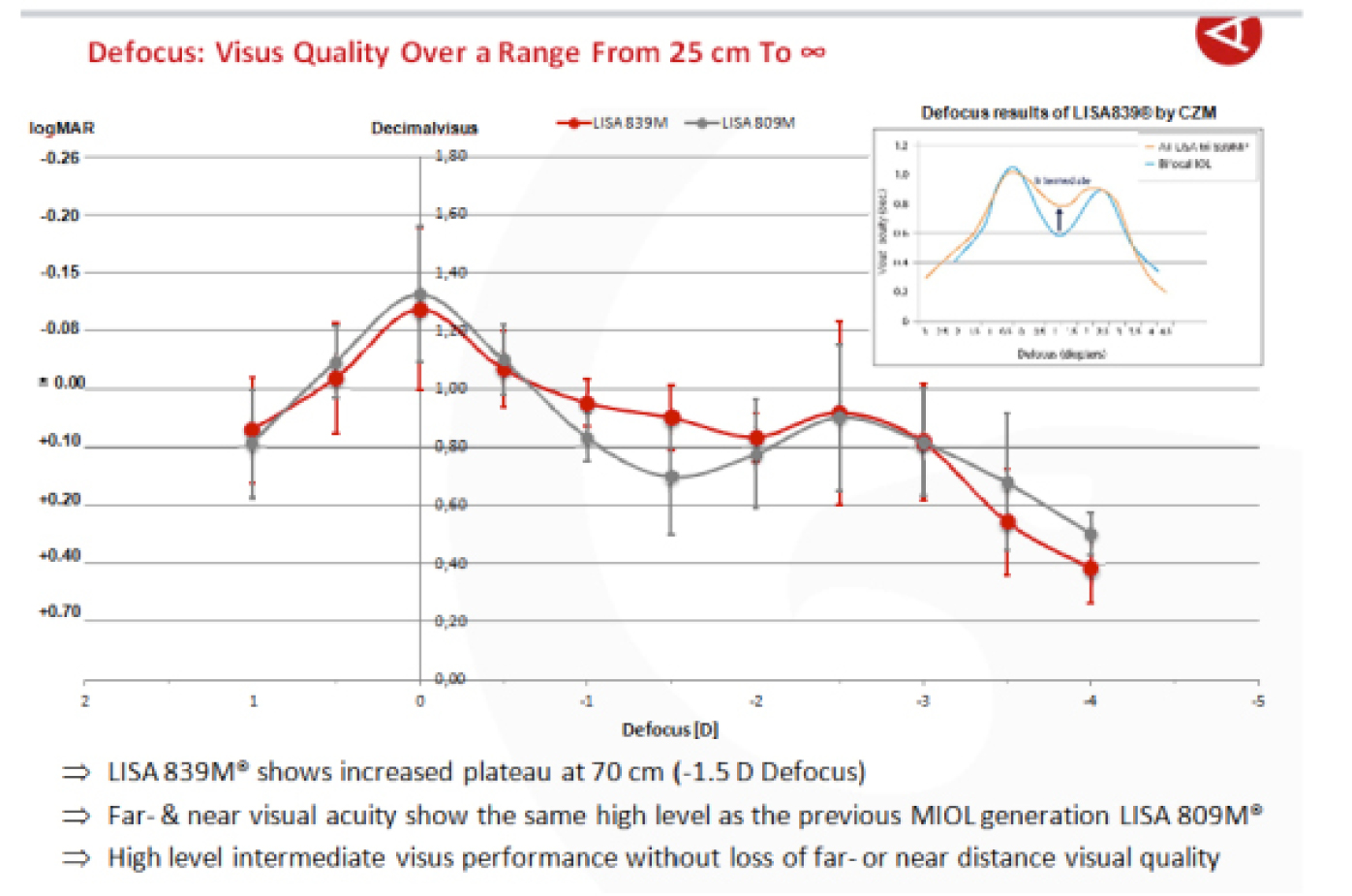
The AT LISA tri 839MP(red) and AT LISA 809M (gray) defocus curves.1
With the AT LISA tri lens design, ophthalmic viscosurgical device (OVD) removal can be a little tricky. However, we have found that by rotating the IOL horizontally to the incision, we are able to easily go under the lens and remove all of the OVD. The ability to rotate the IOL both ways is really advantageous.
Conclusion
The introduction of this new trifocal IOL into our practice has improved our results and increased patient satisfaction, especially in terms of improving intermediate vision and reducing night vision symptoms. Investing the chair time to select the appropriate candidates for this lens remains a priority.
1. Breyer D. Introducing the trifocal AT LISA tri 839MP. Paper presented at: the 26th APACRS Annual Meeting; July 11-14, 2013; Singapore.
