Thus far in the Presbyopia Challenge column, we have been discussing concepts in assessing and correcting presbyopia without delving into any specific technology. In reality, many surgical approaches and technologies have already been utilized to improve our patients’ ability to see both distance and near without glasses.
Thinking in terms of the defocus curve that Jeremy Kieval, MD, presented in the last installment of Presbyopia Challenge, our primary goal is (1) extending the depth of focus while (2) maintaining quality of vision and preventing visual side effects throughout that focus range. How well we meet these two objectives is significantly influenced by the technology that we use. Examples of these technologies include refractive optics, diffractive optics, accommodative optics, and reduction of aperture. In addition to the complexity of optics that each of these technologies brings, there is an increasing complexity of nomenclature associated with designating each technology.
Take presbyopia-correcting IOLs as an example. We have refractive multifocal IOLs, accommodating IOLs, diffractive multifocal IOLs, and trifocal IOLs. We will soon have hyperaspheric IOLs, extended depth of focus IOLs, and extended range of vision IOLs. If the technology was confusing, the naming of technology doesn’t help to clarify things.
So, how does an IOL category get named? Ideally, a convergence of three factors determines the name: technical, regulatory, and marketing. The market-driven recognition and acceptance of a name necessarily depends on what regulatory approvals allow. Regulatory approvals vary from region to region, based on claims supported during the approval process. These claims originate from the technical aspects of the IOL. It all starts with the technical aspects of an IOL design: the mechanism of action and the defocus characteristics.

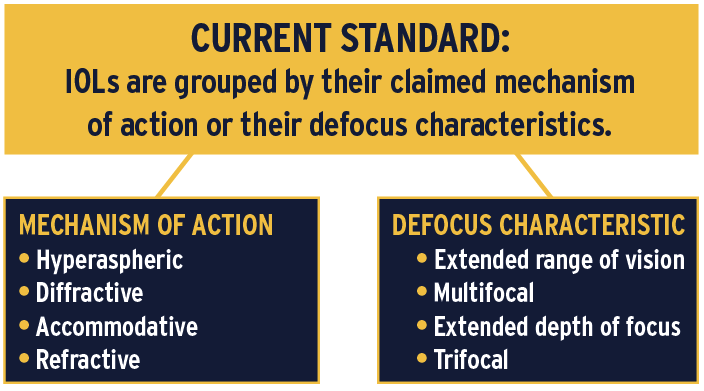
Currently, IOLs are almost arbitrarily grouped by either their claimed mechanism of action and/or their defocus characteristics. That’s why some IOLs are called multifocals (a defocus curve description) while others are called accommodating (a mechanism of action). With the addition of extended depth of focus IOLs and hyperaspheric technology, matters will become even more confusing unless a unifying approach is taken.
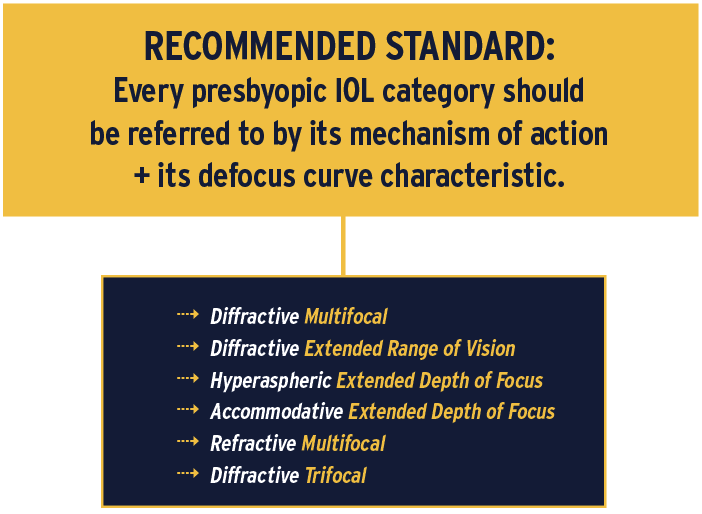
My recommendation is to call IOLs by both. Every presbyopic IOL category should be referred to both by its mechanism of action and by its defocus curve characteristic. For example, multifocal IOLs could be characterized as diffractive multifocal IOLs, and accommodating IOLs could be characterized as accommodating extended depth of focus IOLs. This way, each IOL will be fully characterized by a description of how it works and what it seeks to do.
Of course, prior regulatory approvals will limit the claims and names by which companies can refer to their devices. Indeed, even the concept of extended depth of focus is seeking definition by the FDA. Clearly, the process of naming presbyopia-correcting technology has no simple solutions. Nevertheless, surgeons should start thinking in clear and consistent ways so that we can determine the technology and surgery that will best help our patients—regardless of what it’s named.