
A 31-year-old male presented for a refractive consultation. He was getting married, and the consultation was a gift from his fiancée. He was very nearsighted and wore contact lenses and thick glasses that he had tired of. This patient was hoping that he could improve his prescription enough to reduce his dependence on spectacle correction.
After I examined the patient and took preoperative topographies with the WaveLight Topoloyzer VARIO diagnostic device (Alcon), I explained that I could treat him with this new topography-based technology, which I felt would be the best refractive treatment for him, given his prescription (highly myopic with significant astigmatism). I explained that CONTOURA Vision (Alcon) could treat not only his prescription, but also the irregularities on his cornea.
Pre- and Perioperatively
My staff and I obtained final presurgical topographic images for this patient prior to surgery with CONTOURA Vision, after instructing him to leave his contact lenses out for 2 weeks. On the day of surgery, we treated him with 8.00 D of sphere bilaterly in an uneventful procedure.
Postoperatively
On the first postoperative day, the patient achieved 20/15 UCVA in each eye (20/10 -2 OU SC). At his 2-week follow-up visit, the patient was seeing 20/15 UCVA in each eye separately, and 20/10 UCVA OU (Figures 1–10). At the time of this writing, the patient has zero postoperative symptoms, and he is so happy with his vision that his fiancée has scheduled surgery for herself. While achieving a postoperative vision of 20/10 is unusual in and of itself, achieving it in an eye with -9.00 D of myopia is impressive.
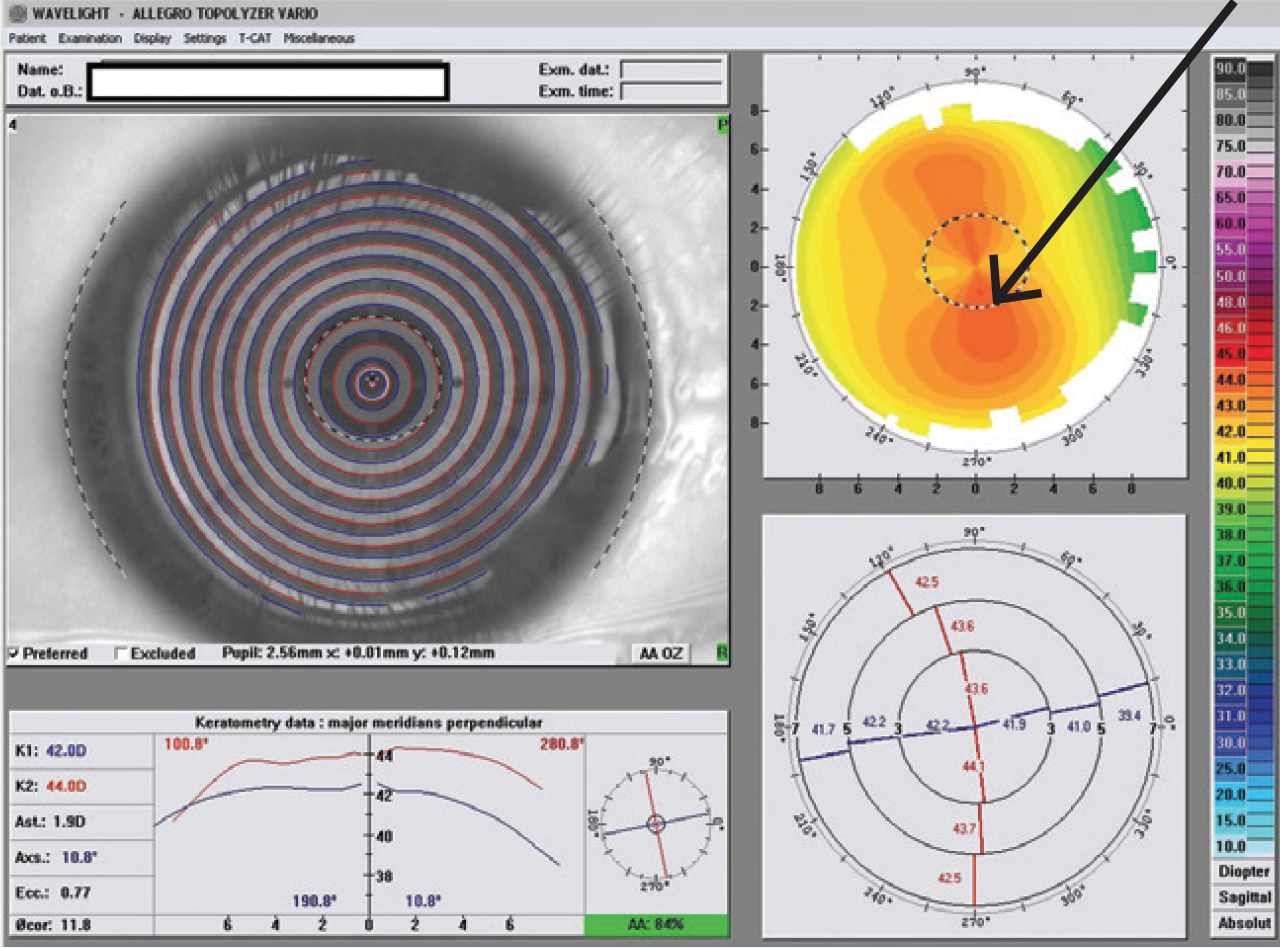
Figure 1. Preoperative topography OD shows WTR asymmetrical astigmatism.
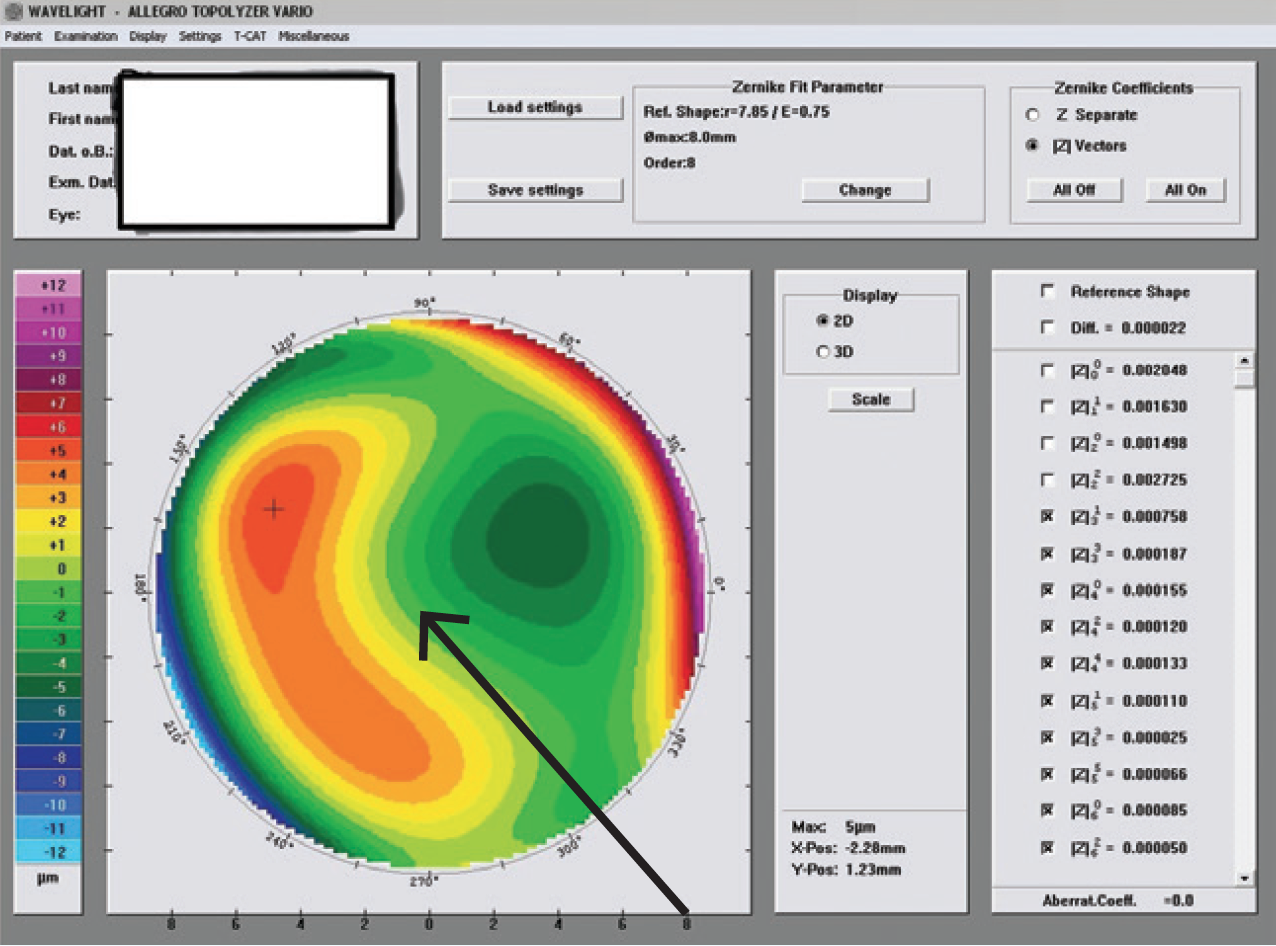
Figure 2. The preoperative Zernicke higher-order aberration coma, OD.
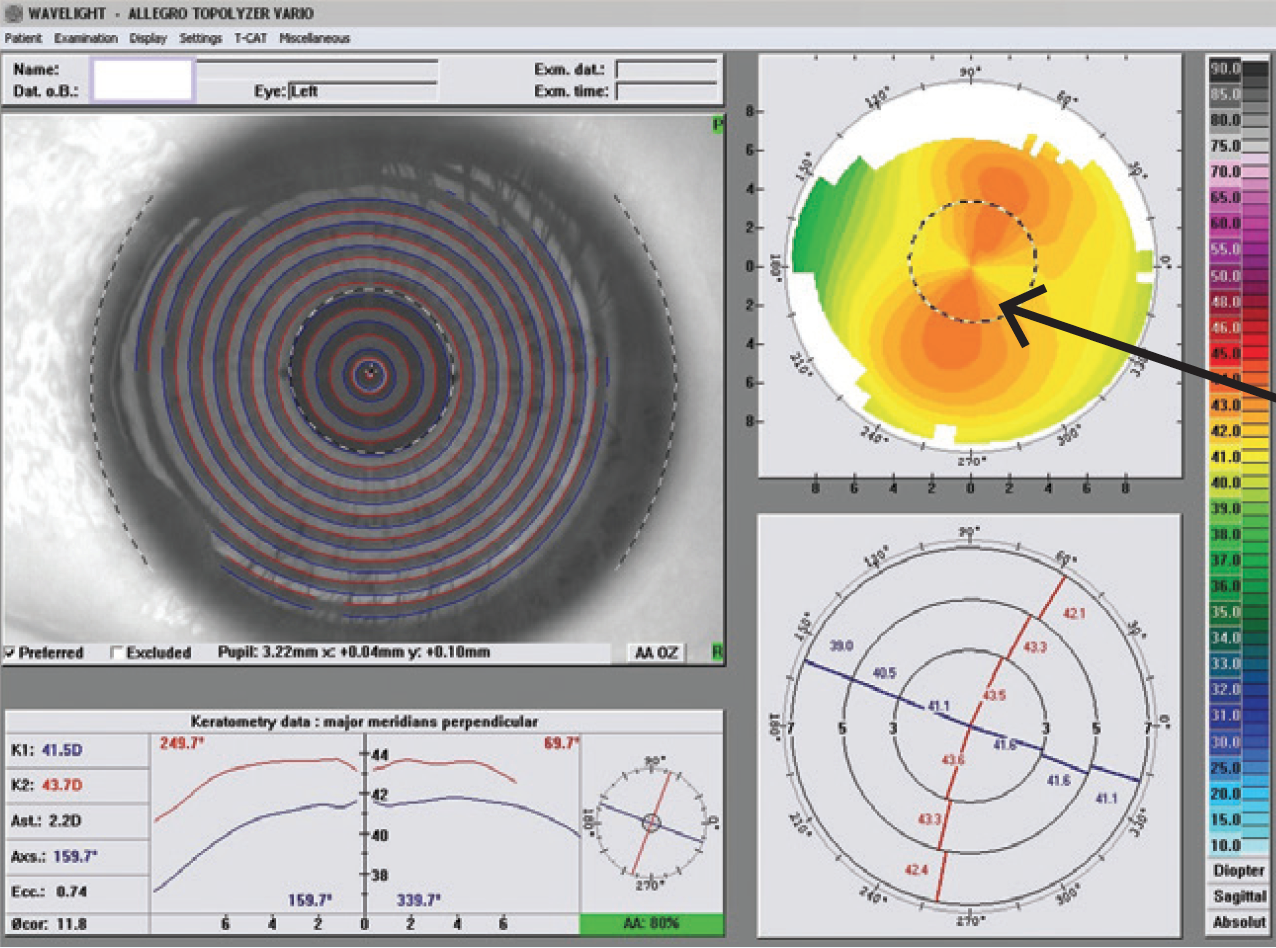
Figure 3. Preoperative topography OS shows WTR asymmetrical astigmatism.
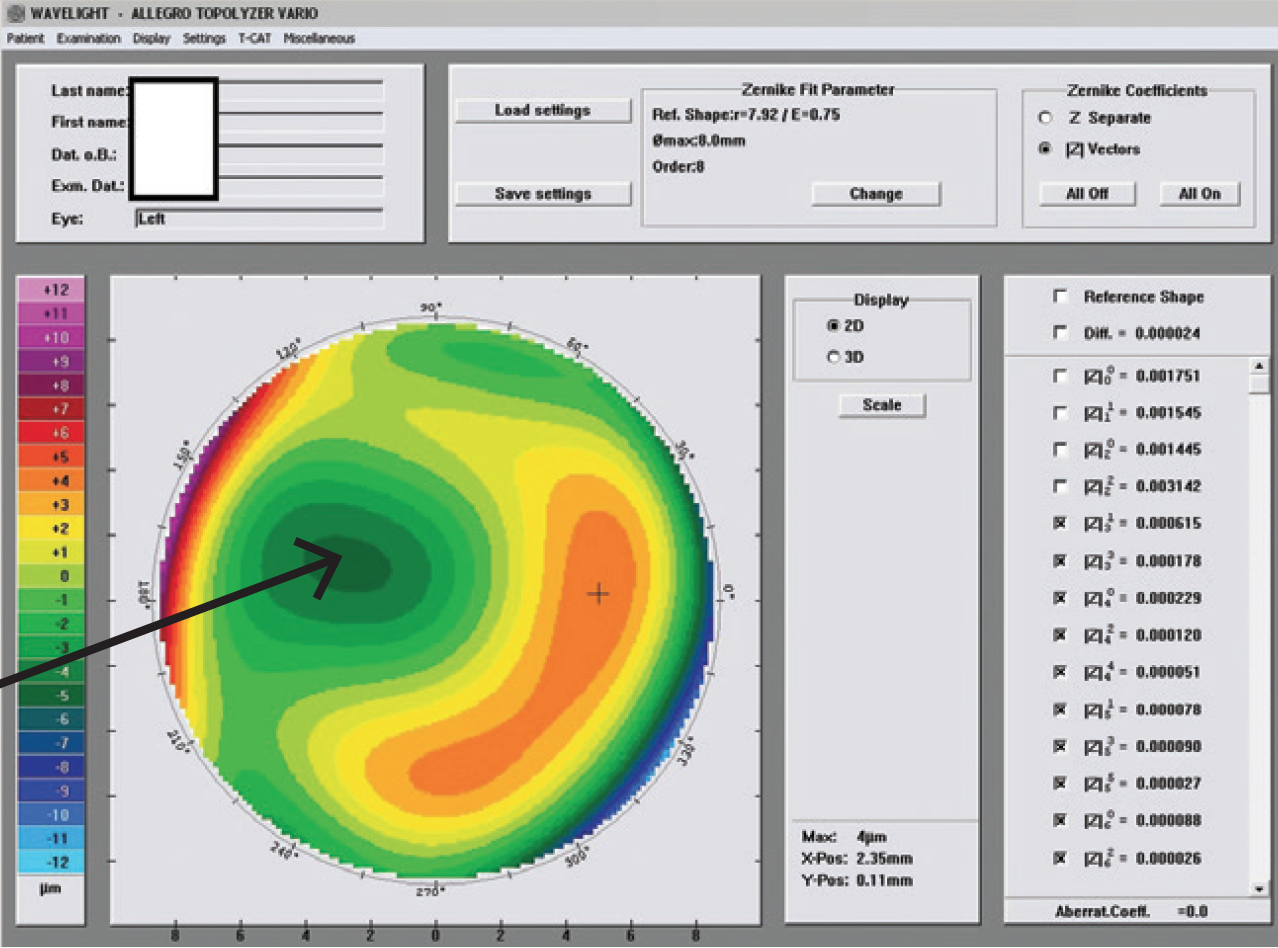
Figure 4. The preop Zernicke higherorder aberrations, OS. Note the coma.
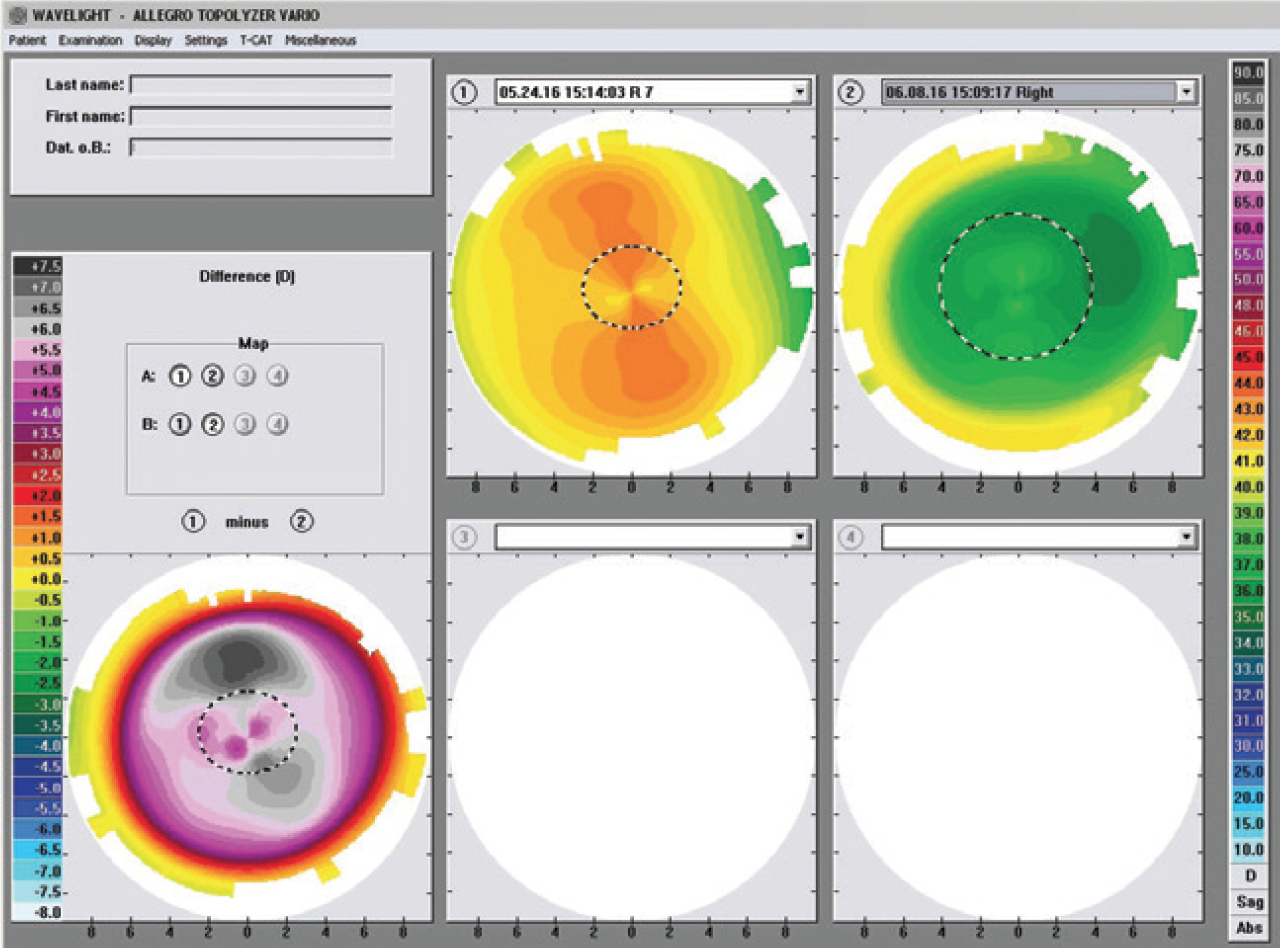
Figure 5. The patient’s maps at 2 weeks postoperatively (comparison images).
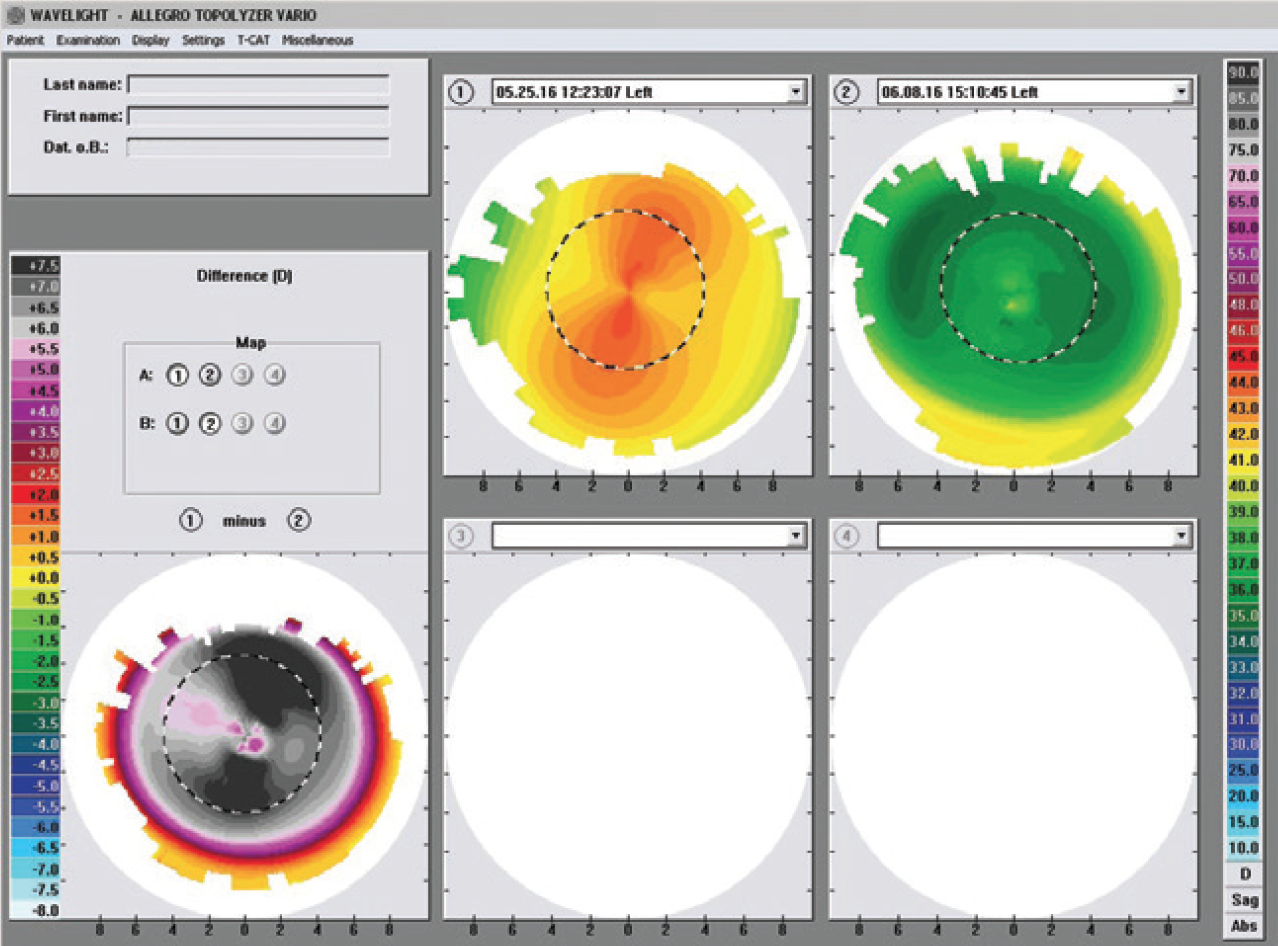
Figure 6. The patient’s maps at 2 weeks postop (higher-order aberrations).
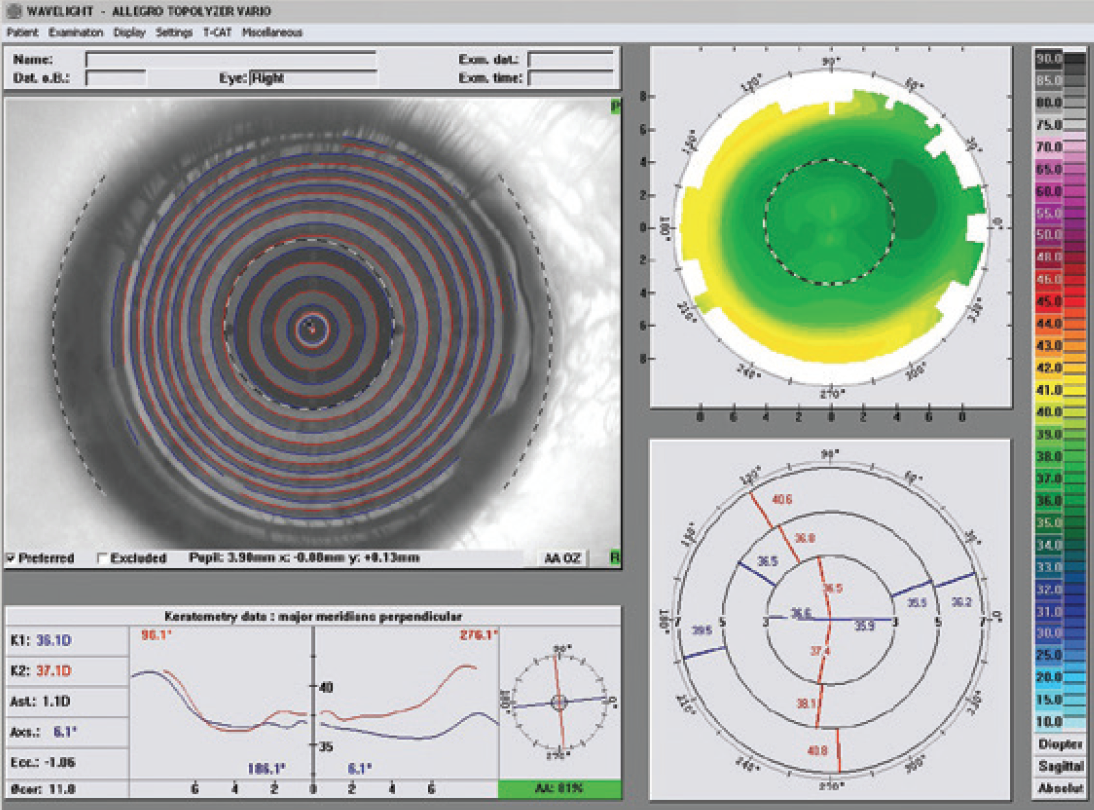
Figure 7. The patient’s topographic maps of the right eye at 2 weeks postoperatively (topographic images).
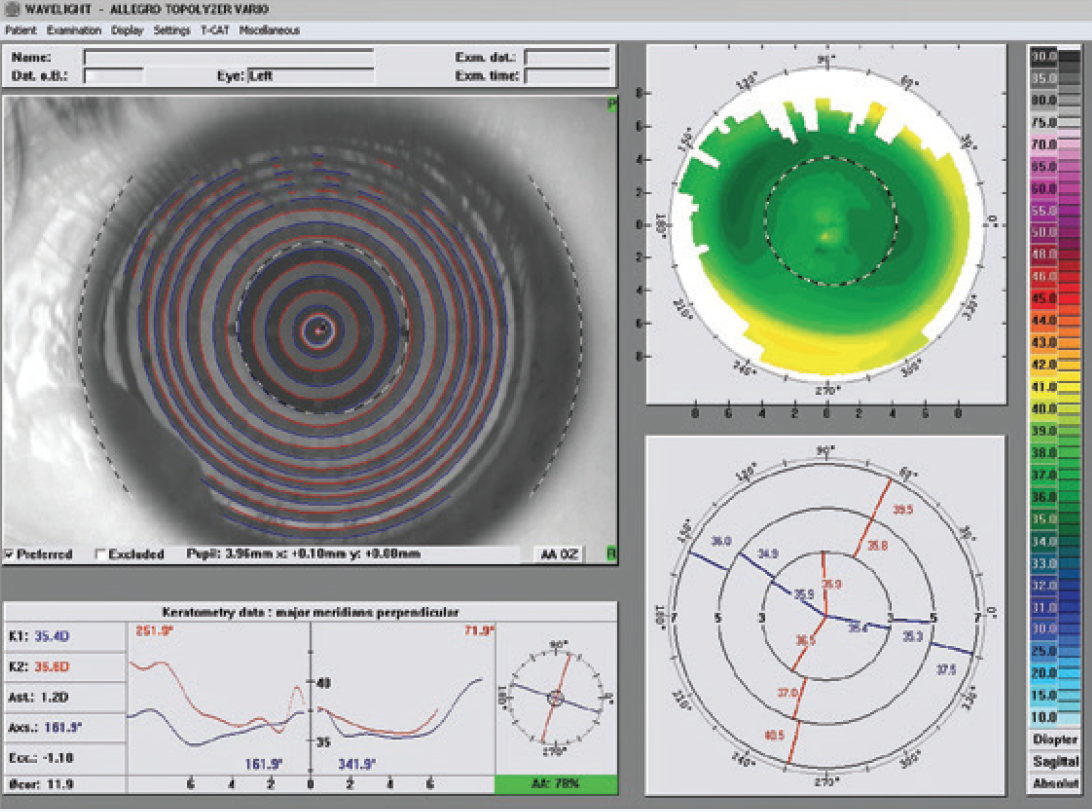
Figure 8. Two weeks postoperatively, left eye.
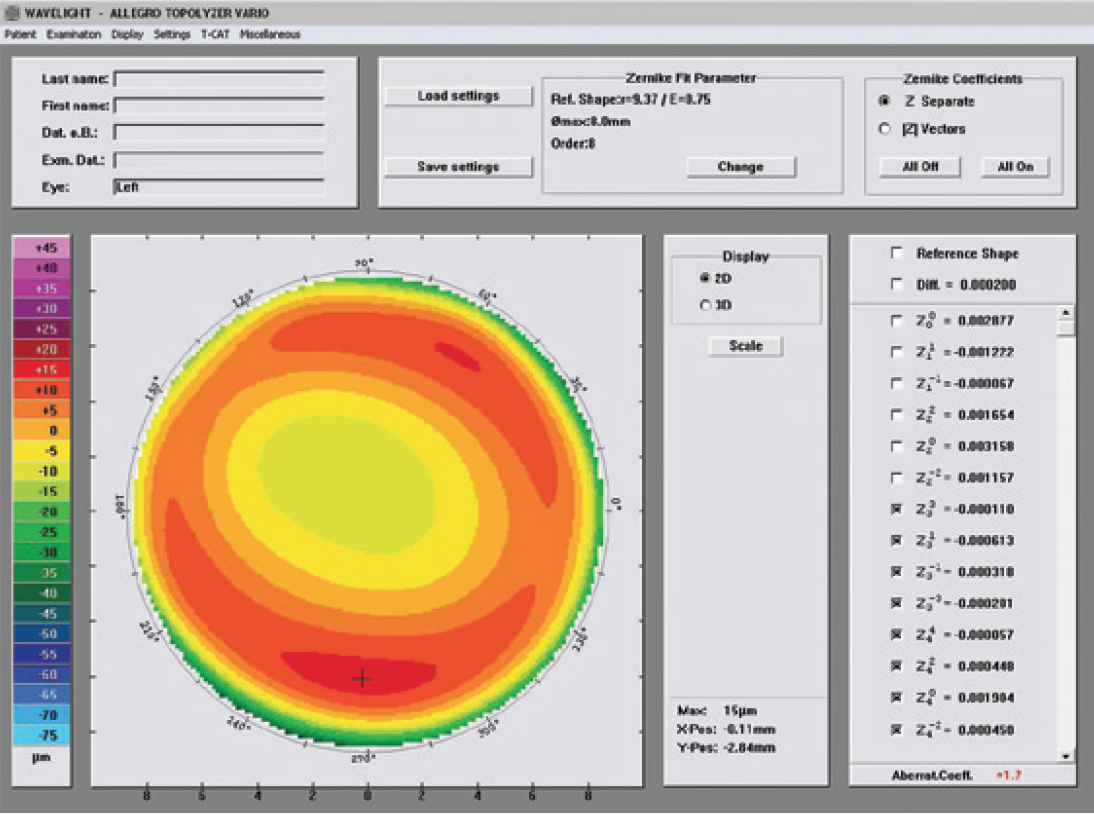
Figure 9. Two weeks postoperatively, left eye.
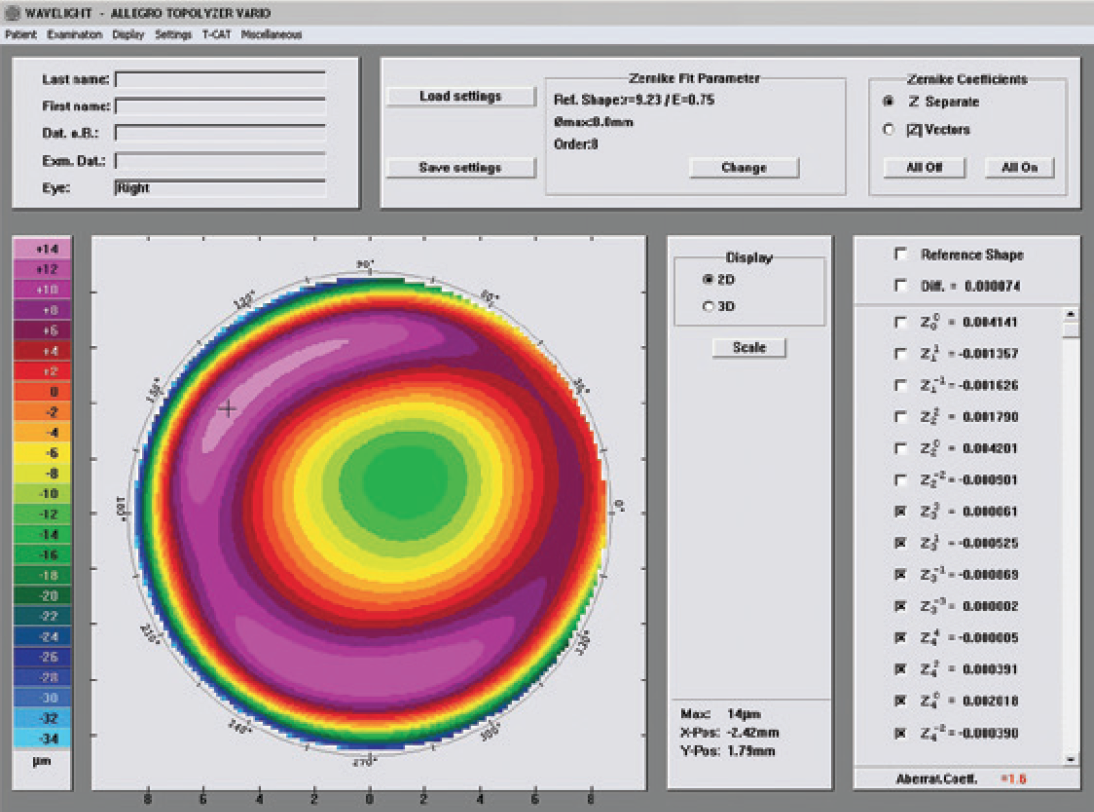
Figure 10. Two weeks postoperatively, right eye.
Discussion
Performing the CONTOURA Vision surgery itself is no different from performing any other LASIK procedure. The preoperative workup and planning are somewhat different, but worth it; I believe CONTOURA Vision results are better than with other treatment algorithms for these types of patients. The CONTOURA Vision procedure differs from wavefront-optimized ablations by using the Q-value of the patient’s own cornea, not a population-average Q-value. Plus, we can center the CONTOURA Vision treatment on the corneal apex rather than the center of the pupil. These factors combine to produce a more precise refractive treatment.