


The CONTOURA Vision (Alcon) system is changing LASIK. The technology enables surgeons to treat each cornea’s unique topographic irregularities in a broad range of LASIK patients, which may produce a better quality of vision. By removing each cornea’s topographic irregularities CONTOURA Vision treatments also benefit patients by reducing night vision problems such as glare and halos.1 That is unique to CONTOURA Vision; a LASIK technology that creates vision higher in quality than anything that has come before. Vision for many patients that is superior to what glasses, contacts, or traditional LASIK can offer. Today, CONTOURA Vision is a practice differentiator, garnering high patient satisfaction and referrals for surgeons who use it.
Outcomes with CONTOURA Vision can be spectacular. In FDA clinical trials and today in open use, CONTOURA Vision outcomes are measurably superior and show noticeably better patient satisfaction compared to standard LASIK. After the procedure in 249 eyes, 92.6% of patients have 20/20 or better uncorrected visual acuity—better than preoperative best-corrected visual acuity in more than 30% of eyes.2 An astounding 1 in 3 patients achieved 20/12.5 or better uncorrected vision. CONTOURA Vision also has lower rates of symptoms associated with LASIK, such as light sensitivity, night driving problems, reading difficulty, glare, halos, and starbursts.1 Given the higher quality of vision that CONTOURA Vision delivers to patients, in a survey of 124 patients, 98% said they would have the procedure again.2
Next-level Technology With Broad Application
CONTOURA Vision takes customized refraction a step further by addressing very specific problems related to corneal topography that had never been fully addressed before. New cutting-edge topography must be meticulously accurate, without shadows, tear film disruption, or other factors that could impair its quality. What used to be an assessment tool is now a surgical guide because the topographic corneal data are sent to the Alcon WaveLight laser and actually used to improve the accuracy of the excimer laser treatment. That’s a true paradigm shift—topographic data not just examined by the surgeon but actually sent directly to the laser as part of the treatment. And as always, the quality of the outcomes starts with the quality of input into the laser.
Once practices master capturing WaveLight Topolyzer VARIO Diagnostic Device (Alcon) images, the rest of the CONTOURA Vision process is seamless (Figure 1). Through a highly visual process, the software helps technicians and surgeons evaluate the quality of the images, so it is easy to pick the four images required for surgery. We can now look at exquisitely detailed corneal topography, isolate the impact of any topographic aberrations on the cornea, and decide how to integrate those aberrations into the refraction. Finally, the laser will have the actual 22,000 topographic data points for each eye’s treatment, a huge improvement over simply imputing a steep K and a flat K. The 22,000 keratometric data points are much better than 2 simple K readings.
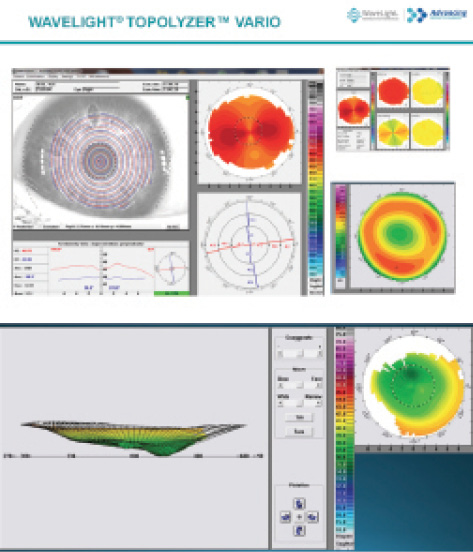
Figure 1. The WaveLight Topolyzer VARIO Diagnostic Device.
CONTOURA Vision is not a premium surgery for just a few patients. Patient selection is similar to LASIK or PRK, and anyone who falls within the established guidelines (up to -8.00 D sphere, up to -3.00 D cylinder, and a spherical equivalent no greater than -9.00 D) can potentially be a CONTOURA Vision patient. Even patients with low refractions benefit from CONTOURA Vision, because everyone has topographic aberrations in the cornea that affect visual performance. However, we sometimes need to rule out patients if we think that corneal scarring or another challenge will make it impossible to acquire reliable images. I use CONTOURA Vision for all of my eligible patients and on most days 80% to 90% of my patients are treated with CONTOURA Vision. Yet 100% of my patients benefit from it. How so? Because even if a patient can’t have CONTOURA Vision, we are still able to capture iris recognition data, which is sent to the WaveLight laser’s tracker. This allows perfect axis placement of astigmatic treatments in WAVEFRONT OPTIMIZED treatments. Hyperopic patients benefit because the Topolyzer VARIO data can identify the true corneal vertex. Hyperopic treatments can thus be centered on the pupil center or the corneal apex depending on surgeon preference for each eye. Tangible benefits from having your diagnostic technology “talk” directly to your laser.
Capture the High-quality Measurements You Need
To optimize the outcomes of refractive surgery with CONTOURA Vision, we need to capture high-quality images with minimal shadowing and healthy tear film. My staff and I follow these five steps:
1. Ensure the ocular surface is clear and consistent. Because the Topolyzer VARIO is a Placido disc measurement that relies on rings reflected onto the corneal surface, it is important to have a healthy, uncompromised ocular surface. In preparation for these measurements, we have patients stop wearing soft contact lenses for 1 week, or gas permeable lenses for 3 weeks. We also perform the Topolyzer VARIO measurements first, before any other testing is done that requires staring or other actions that can disrupt or distort the tear film or corneal surface.
2. Position and coach the patient. Patients have a role in capturing the best CONTOURA Vision images, so our technicians give patients a 30-second overview of what to expect before they begin. Technicians explain that nothing uncomfortable or surprising (no puff of air) will take place during the measurements.
Body positioning is very important, because if patients are uncomfortable, they will move a lot, which makes it difficult to capture a good image. Patients should be sitting upright in a comfortable position, and we do not want them to sit back in between measurements (Figure 2). Patients can help optimize their ocular surface by keeping their eyes closed between measurements. When the technician is ready to capture a measurement, they instruct patients to do three quick blinks, open their eyes wide with their eyebrows up, and focus in the center of a little yellow “donut” (fixation target). If it takes longer than 4 to 5 seconds to capture an image, technicians tell the patients, “blink, blink, blink, and brows up,” and they try again.
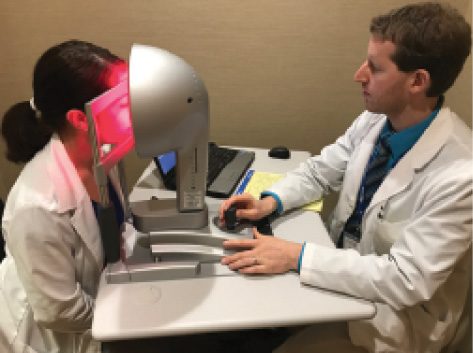
Figure 2. A technician using the Topolyzer VARIO system with a patient.
3. Position the eyes for optimal image capture. The right positioning helps ensure that we get the most data possible for CONTOURA Vision treatment. First, we adjust the table height so patients are comfortable because uncomfortable patients naturally shift around and need to be repositioned. To prevent shadowing from the nose, we measure the right eye with the head turned (never tilted) slightly to the left, and measure the left eye with the head turned slightly right. Using the forehead spacer is also important because it helps push the forehead back ever so slightly for better superior exposure. Technicians do a quick eye-to-eye test before taking the first measurement on the right eye or left eye, in order to help ensure there is no cyclotorsion related to head tilt. Sometimes having a second technician lift the eyelid from the side helps as well (Figure 3).
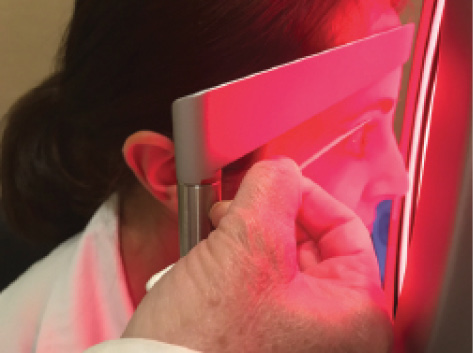
Figure 3. The right positioning helps ensure that we get the most data possible for CONTOURA Vision treatment.
4. Capture six images for the CONTOURA Vision procedure. Optimally, we need four images to perform the CONTOURA Vision procedure. For patients whose measurements fall within the criteria for CONTOURA Vision surgery (up to -8.00 D sphere, up to -3.00 D cylinder, and a spherical equivalent no greater than -9.00 D), my technicians aim to capture six images. This allows me to rule out outliers, such as images with variations from compromised tear film or missing data (lids, lashes, or nose shadows) during the comparison process. However, I will still proceed with CONTOURA Vision in many cases if we capture fewer than 6 images but those that are captured are of a high quality.
5. Gather measurements for other refractive surgeries. When patients fall outside the CONTOURA Vision indication, the Topolyzer VARIO measurements are still valuable. Iris registration can be used for other procedures. I also export data from the Topolyzer VARIO (patient demographics, iris registration, keratometry, and corneal vertex measurement) for any WAVEFRONT OPTIMIZED procedure I perform using the WaveLight EX500 Excimer Laser (Alcon). This increases our efficiency on OR days as the data will not need to be entered into the laser “on the fly.”
Analyze and Select the Best Images
Once we capture images for the CONTOURA Vision procedure, my technicians follow an interactive image analysis process, eliminating outliers and verifying that measurements are consistent and reliable (Figure 4). From the patient’s six captures, they select four high-quality images for either the CONTOURA Vision procedure or for iris registration alone.
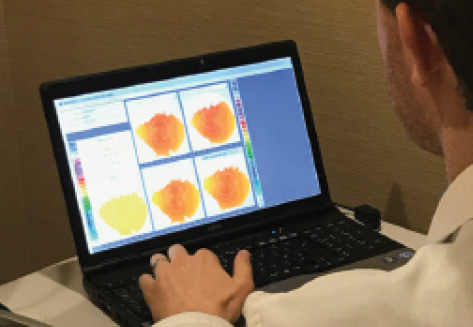
Figure 4. Once we capture images for the CONTOURA Vision procedure, my technicians follow an interactive image analysis process, eliminating outliers and verifying that measurements are consistent and reliable.
First, we compare measurements for consistency and reliability of +/- 0.75 D. Using comparison maps of the treatment area in the Compare Images Display on the Topolyzer VARIO, we look at four images on the screen. We choose the scan with the best tear film/topography image as a baseline for comparing Topolyzer VARIO images. To compare other images to that baseline, we check from the pupil to the mid-periphery to make sure that the difference is less than 0.75 D. After discarding the outliers, we pull up additional scans and make the same comparison.
Next, the Analyzer Area tool helps us ensure we have the data we need. It calculates the data available for 5.50 mm and 6.50 mm optical zones. The Optical Zone Analyzer section on the Overview page shows the optical zone for the eye, split into inferior, superior, temporal, and nasal quadrants (Figure 5). The software marks each quadrant in red or green. Green check marks tell us that there is enough data in the optical zone for CONTOURA Vision and iris registration. In addition, a green “P” means preferred (for the CONTOURA Vision procedure) and a green “R” indicates good iris registration.
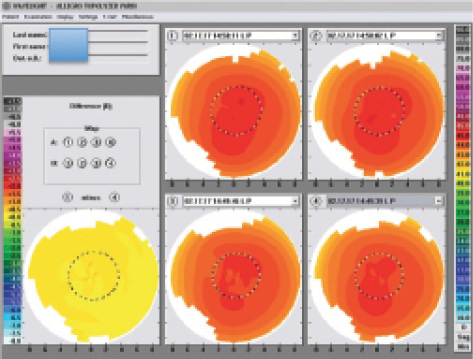
Figure 5. The Optical Zone Analyzer section on the Overview page shows the optical zone for the eye, split into inferior, superior, temporal, and nasal quadrants.
If the examination is less than perfect, the screen will display a red “X” and show which quadrant or quadrants have insufficient data. For example, data may be missing from the superior region if the eyelashes cast a shadow, or the nose may have a shadow in the nasal quadrant.
Images should have 90% or higher AA OZ in the 6.50 OZ and pupil border recognition within 0.1 mm or 100 μm of the baseline image. Patients typically will have several scans with sufficient data, but if, for example, the 5.50 mm optical zone has 100% of the data, while 6.50 mm is missing data but is still over 90%, we can manually change the image to “preferred” for the CONTOURA Vision procedure. Any scans below those thresholds are not usable. Alcon’s trainers are excellent and can help explain all of this thoroughly. In practice, it is not difficult.
Calculate CONTOURA Vision Treatment
Once the technicians have a good set of images for surgery, I calculate the laser refractive treatment for the CONTOURA Vision procedure. It begins with checking the reproducibility of imported measurements. Once my technicians send the selected scans to the laser, I have the opportunity to double-check them for accuracy. At the planning station, I look at the images in the Raw Data Sagittal view, comparing the appearance of the corneal topographies and eliminating any extreme outliers. Inspect the K values, axes, Q values, and pupil sizes, if necessary. This usually takes me about 30 seconds or less.
Watch Now
Watch as Dr. Lobanoff describes strategies for implementing CONTOURA Vision in practice.
I can dig deeper into the data behind the images if needed, but generally, this simplified approach is very effective. Once I approve the scans and removed any scans that the technician may have missed, I am ready for the next step.
Advancing to the next screen, I input the patient’s specific treatment data: manifest refraction, vertex distance, K values, pupil size, and pachymetry results (Figure 6). The third page in the planning process is where I can calculate the patient’s final treatment. In the table at the top of the page, the top line displays the manifest refraction that was inputted on the previous screen. The second line shows the highly accurate measured refraction and cylinder axis of the astigmatism found by the Topolyzer VARIO. (Note: the Topolyzer VARIO is incapable of determining the sphere, so this figure should be disregarded.) On the third line, known as the “Modified” line, I enter the final, nomogram-adjusted treatment chosen for the eye.
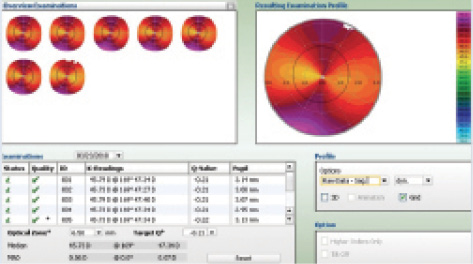
Figure 6. This screen shows the patient’s specific treatment data: manifest refraction, vertex distance, K values, pupil size, and pachymetry results.
In making my final choice for treatment, I consider which nomogram to use and whether I should make an age adjustment. I can also dig deeper into the topographic pattern found on the cornea and think about how this can affect the refraction. To see how the CONTOURA Vision procedure will remove these aberrations to provide a smoother, more regular corneal surface, I enter 0 in the modified sphere and cylinder boxes. The resulting ablation profile shows only the anterior corneal topographic aberrations (Figure 7). Understanding how the aberrations in this profile can influence vision, I feel confident in treating patients with CONTOURA Vision.
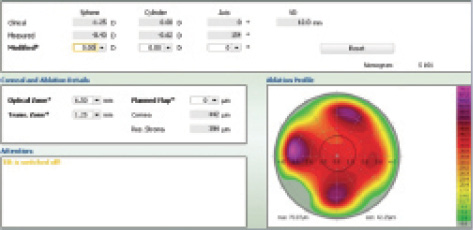
Figure 7. This ablation profile shows only the anterior corneal topographic aberrations.
Because I have been using CONTOURA Vision for more than 2 years, and we track our outcomes, I am able to individualize patients’ treatment calculations, when needed, based on various criteria. This is the “art” of working with CONTOURA Vision, and it comes with experience. However, for surgeons who are new to the procedure, I recommend following the straightforward calculations given by Alcon, which are based on the company’s most current data. Start simple and straightforward, then advance with more complex treatments as you gain experience and confidence with the technology.
CONTOURA Vision Training and Implementation
With CONTOURA Vision, there are some additional steps versus standard WAVEFRONT OPTIMIZED LASIK, where we simply enter refractions and two K values into the laser to guide surgery. We are going from using 2 K values to 22,000 to help achieve better results. Our technicians have to take quality, reproducible images, and surgeons have to take a more in-depth look at the corneal topographic irregularities. Once we began using this approach in my practice, my staff and I quickly became confident, and now it adds only a little extra time. But that extra time and effort are worth it in my practice, because better outcomes with higher quality of vision leads to happier patients and more referrals. We take pride that we are offering excellent refractive treatments for our patients. It is how we separate ourselves in a competitive market.
Like any paradigm shifting technology, CONTOURA Vision required a period of transition. The Alcon team trained our surgeons and staff very thoroughly and conveniently. The Alcon trainer spent a full workday with our technicians, training them to capture and analyze scans, observing their work with patients, and answering questions. Next, Alcon practiced surgical planning for CONTOURA Vision procedures with our surgeons, and they were there on surgery day to make sure everything went smoothly. The trainers are available to answer questions, visit additional surgery days, or do refresher training for technicians and new staff. The instruction and support helped us implement the CONTOURA Vision measurement process and procedure very quickly and confidently.
After just a few weeks of practice, CONTOURA Vision did not have a major impact on patient flow at the clinic or surgery center. Because CONTOURA Vision is a practice differentiator, Alcon has also given us some pointers so we could position ourselves to turn patient satisfaction into referrals for the procedure. CONTOURA Vision helps us deliver a game-changing procedure that reduces side effects commonly associated with LASIK, and we want patients in our community to know that we offer those advantages.
1. Stulting RD, Fant BS, The T-CAT Study Group. Results of topography-guided laser in situ keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg. 2016;42:11–18.
2. At 12 months: Summary of safety and effectiveness data, WaveLight ALLEGRETTO WAVE Eye-Q Excimer Laser System and the ALLEGRO Topolyzer. September 27, 2013. Available online: http://www.accessdata.fda.gov/cdrh_docs/pdf2/P020050S012b.pdf
