

Differences between CONTOURA Vision (Alcon) and other LASIK diagnostic procedures were clear from the start. When you read that after a CONTOURA Vision procedure, over 30% of eyes have UCVA that exceeds preoperative BCVA,1 you know that CONTOURA’s WaveLight Topolyzer Vario (Alcon) component is producing measurements that are different from manifest refraction. The highly individualized topography-guided procedure produces excellent visual outcomes while reducing symptoms associated with LASIK, telling us that it, too, is different from previous technologies.1
When I began using CONTOURA Vision 12 months ago, I saw these differences firsthand. I did not embrace the system immediately. Instead, I spent time double-checking CONTOURA Vision against other technologies and cautiously integrating it into my treatment protocols. Over a 6-month period, I grew very satisfied with both the accuracy of the data and the surgical outcomes as well as surprised at the system’s ability to correct cases previously untreatable with LASIK. I learned to trust measured over manifest refraction and put my well-earned faith in the technology.
After CONTOURA Vision, patients are noticing vision clarity and detail that are very impressive, results in line with what the FDA study showed. I recently treated a 47-year-old dentist who had suffered with irregular astigmatism for years. His glasses and contact lenses were designed for “normal” patients with “normal” linear astigmatism. Because his astigmatism was not perfectly linear on topography, glasses and contacts helped his vision but did not perfect it. Following treatment with CONTOURA Vision, he was thrilled with his crisp vision and realized how much detail he had been missing.
“Now, even off-the-shelf reading glasses are amazing! It is as if I am wearing surgical loops,” he told me. He also notes that he no longer sees starbursts while driving.
Here, I share three cases in which I used CONTOURA Vision during this learning curve period, illustrating how the system compared to other tests and how it performed in surgery. The cases range from a straightforward procedure to a case that was untreatable with other standard LASIK technologies. Note: Because CONTOURA Vision requires surgeons to treat in minus cylinder, all refractions are presented in minus cylinder to prevent confusion.
Case 1: Close Manifest and Measured Astigmatism
This is an example of the simplest and easiest type of case for using CONTOURA Vision. The patient is a 31-year-old man with mild myopia and low astigmatism. The manifest refraction (-3.00 -0.50 x 25 20/15) matched well with Vario measured cylinder for both magnitude and axis (-0.34D x 5) (Figure 1A). Orbscan (Bausch + Lomb) measurements were -0.2D x 15 (Figure 1B).
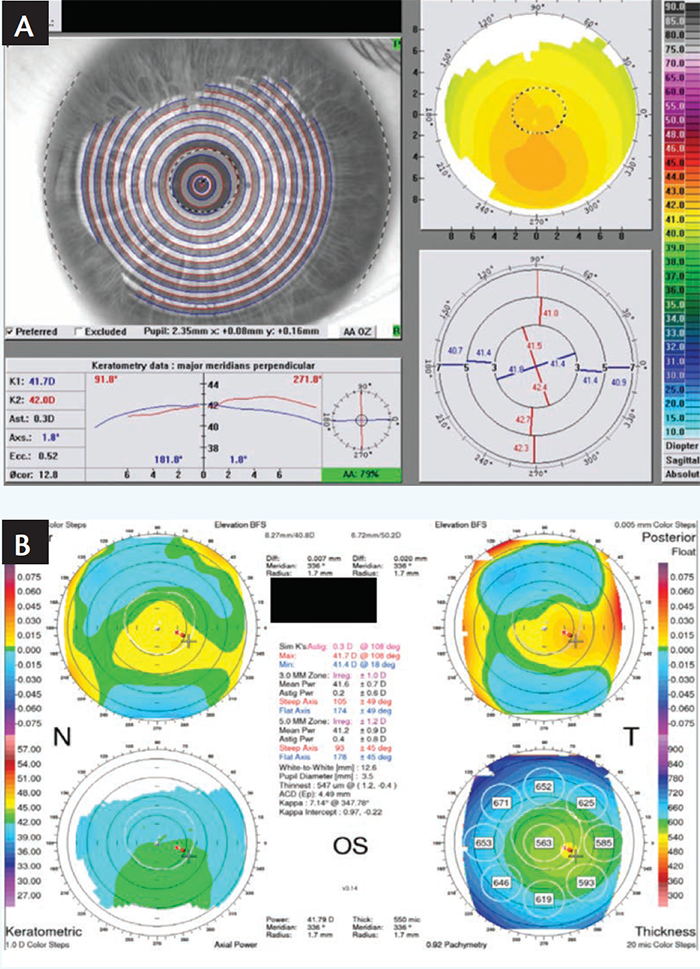
Figure 1. Preoperative Vario scan (A) and Orbscan (B) of a patient with mild myopia and low astigmatism.
On my CONTOURA Vision treatment screen, I looked at the Vario measurements and zeroed out the sphere and cylinder treatments on the “Modified” line. This triggered the system to display the pure topographic treatment planned by CONTOURA Vision on a color map, which indicates the amount of tissue to be removed in different areas (Figure 2).
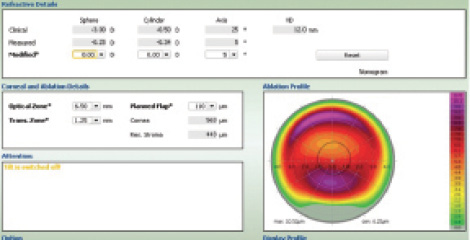
Figure 2. The CONTOURA Vision treatment screen.
The final treatment programmed for this patient was -3.25 -0.34 x 5 (the measured, not the manifest refraction). Treatment was perfectly centered thanks to the highly sensitive pupil-tracking technology. One day after surgery, the Vario scan showed that the treated cornea of the patient’s left eye had smooth, even contours (Figure 3). UCVA was 20/20 day 1 and 20/15 at 2 months, with plano sphere.
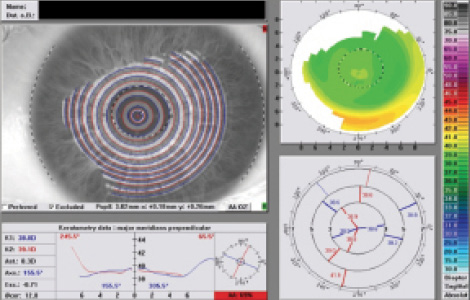
Figure 3. One day after surgery, the Vario scan showed that the treated cornea of the patient’s left eye had smooth, even contours.
Case 2: Measured Astigmatism Exceeds Manifest
I commonly encounter cases where the manifest refraction shows less astigmatism than the Vario measured refraction. I must decide whether to fall back on my previous LASIK experience and treat the manifest or trust the Vario measurement and treat based on its recommendation.
In one such case, a 39-year-old man with moderate myopia and no astigmatism on manifest (OS -4.50 sph 20/15) showed measured astigmatism with Vario (OS -0.99 x 174). In the early stages of using CONTOURA Vision, I found it important to prove to myself that the Vario measured astigmatism was “real” when it differed from the manifest. To verify the measurement, I would compare the Vario’s results to those of a second topographer. It is hard to break years of LASIK experience, and trusting measurements over manifest feels somehow “wrong” at first. No surgeon wants to make a mistake and treat a full 1.00 D of cylinder not seen on manifest. Satisfied with the verification, I learned to trust the technology and treat the true measured astigmatism when using CONTOURA Vision.
In this case, the Orbscan (OS -1.00 x 1) verified the Vario measurements. The Vario and the Orbscan topographers both showed about -1.00 D of cylinder at an axis of about 180° (Figure 4). This assured me that the astigmatism measured by Vario was correct, despite the manifest showing a purely spherical correction.
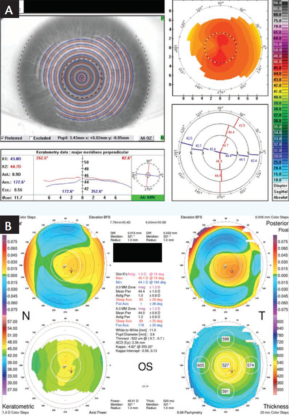
Figure 4. Preoperative Vario scan (A) and Orbscan (B) of a patient with moderate myopia.
I examined the sagittal images of multiple Vario scans for the left eye and found them to be of good quality and in close agreement (Figure 5). On the CONTOURA Vision treatment screen, I zeroed out the sphere and cylinder and viewed the purely topographic treatment that CONTOURA Vision would place on the eye.
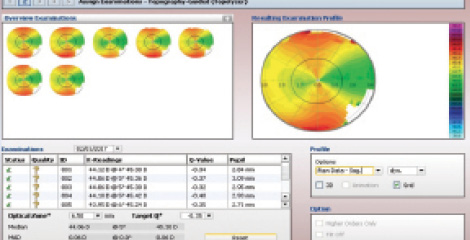
Figure 5. Sagittal images of multiple Vario scans of the patient’s left eye.
The ablation profile showed why the manifest showed no astigmatism while Vario did. Looking at the topographic treatment map, two of the three purple areas where CONTOURA Vision was planning the most tissue removal were located in a vertical line. These elevated areas bend light as if they are cylinders. Because the axis of these raised topographic areas was located at 90° but the true Vario measured astigmatism was located at 180°, the two counterbalanced one another (Figure 6). Thus, the image reaching the retina (the manifest) showed sphere only and no astigmatism.
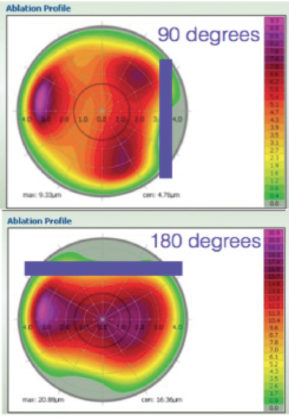
Figure 6. Topography treatment map versus Vario-measured cylinder treatment only.
Treatment was programmed at -4.13 -0.75 x 174, slightly less than the -0.99 x 174 that the Vario had measured. At the time, I did not trust the technology enough to treat 1.00 D more than manifest. This was a mistake. Three months after surgery, the manifest refraction was OS plano -0.25 x 160 20/15. With the topography treated and perfected by CONTOURA Vision, the true cylinder was reflected in the manifest. Had I treated the full -0.99 measured by Vario, the patient would not have had a residual -0.25 at 160. Now I trust the technology and treat the full magnitude and axis that Vario measures to remove the topographic abnormalities of a cornea.
UCVA for this patient was 20/20 at day 1 and 20/20+1 at 3 months. Vario scan showed a beautiful, smooth topographic contour to the cornea with virtually no astigmatism or irregularities. With the topographic abnormalities treated, there was nothing to counterbalance the true cylinder that remained on the cornea. The postoperative Vario scan measured 0.30 D cylinder at 172.4°, very close to the manifest of 0.25 D of cylinder at 160 (Figure 7).
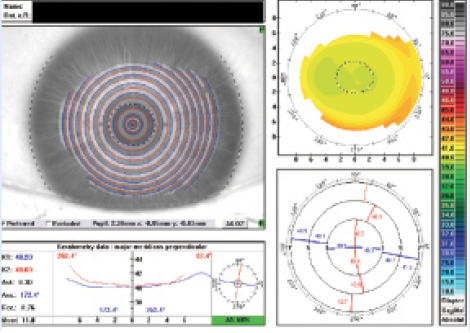
Figure 7. Postoperative Vario scan measured 0.30 D cylinder at 172.4°, very close to the manifest of 0.25 D of cylinder at 160.
Case 3: Choosing Measured Over Manifest
In another case where the manifest astigmatism and Vario measured astigmatism varied, a 28-year-old man had an OD manifest refraction of -6.75 -0.50 x 175 sph 20/15-2, compared to a Vario measurement of -1.50 D at axis 1.5°. Orbscan measured -1.10 D at axis 30 (Figure 8). Once again, I had to make the critical decision to treat based on the manifest cylinder or the Vario measurements.
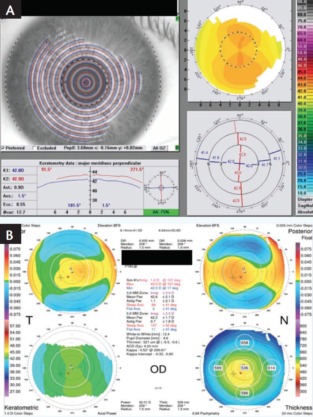
Figure 8. Preoperative Vario scan (A) and Orbscan (B) of a 28-year-old patient.
By removing the sphere and cylinder from the topographic treatment map, surgeons can see an isolated view of the topographic abnormalities that CONTOURA Vision will treat. In this case, this view showed why the manifest cylinder was different in magnitude than the Vario measured cylinder. While some of the topographic abnormalities were mimicking a minus cylinder at 180°, more abnormalities mimicked a minus cylinder at 90°. The topographic abnormalities at the 90° axis counterbalanced both the topographic abnormalities at the 180° axis and the true corneal cylinder measured by Vario. The result was the manifest, which showed astigmatism lower in magnitude than that measured by Vario (Figure 9).
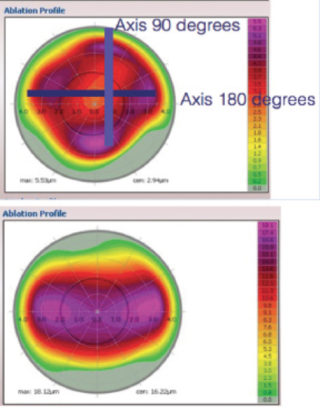
Figure 9. Topography treatment map versus Vario-measured cylinder treatment only.
CONTOURA Vision treatment was programmed to -6.40 -1.00 x 2. Here the spherical portion of the treatment was purposely reduced below the manifest sphere. Because I increased the treated negative cylinder above the manifest negative cylinder, I needed to reduce the spherical treatment by one half the delta (change) in cylinder to keep the spherical equivalent of the treatment equal to the spherical equivalent of the manifest. A small adjustment was also made to the sphere based on the nomogram for my Wavelight Ex500 Excimer Laser (Alcon).
UCVA was 20/20 at day 1. At 1 month, OD UCVA was 20/20, and OD manifest refraction was plano +0.25 x 05 20/20. The 1 month postoperative Vario topographic analysis showed how CONTOURA Vision treatment left a smooth, beautiful topographic contour to the cornea with virtually no topographic abnormalities remaining. Vario’s postoperative scan shows the pupil marked in a hashed line of black and white, with the circular myopic treatment pattern on the vertex of the cornea, not centered on the pupil (Figure 10). This is a key feature of how CONTOURA Vision delivers such exceptional results. The Orbscan topography taken 1 month postoperatively showed perfection in the axial power map.
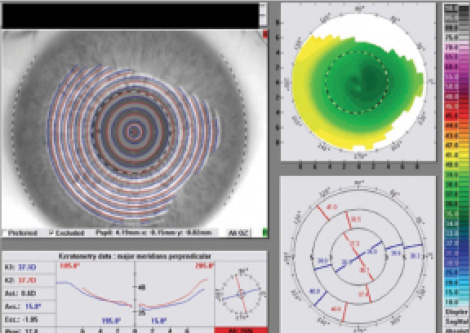
Figure 10. Vario’s postoperative scan shows the pupil marked in a hashed line of black and white, with the circular myopic treatment pattern on the vertex of the cornea, not centered on the pupil.
CONTOURA Vision Inspires Confidence
Every cornea has some topographic abnormalities, but in the past our standard or wavefront-optimized treatments left them in place. CONTOURA Vision treats the cornea completely.
We all want to routinely boost LASIK visual outcomes while reducing the residual symptoms of the procedure. To acquire this capability, we need to use topography-guided treatments such as CONTOURA Vision. To best use CONTOURA Vision, we need to make a mental leap and trust measured refraction over the manifest refraction we have relied on for so long. It is not easy to do that at first, but if you learn to trust the technology, CONTOURA Vision will improve your patients’ results. Better results and happier patients will convince you to embrace this next-generation technology with confidence.
© 2018 Novartis 9/18 US-WVL-18-E-1953
1. Stulting RD, Fant BS; T-CAT Study Group. Results of topography-guided laser in situ keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg. 2016;42:11–18.