


Telemedicine is often touted as the way of the future, but it was not until recently that ophthalmologists felt a pressing need to implement the practice into routine care. Now, in the age of COVID-19, telemedicine is the safest and most secure way for us to connect with high-risk patients and to minimize exposure to the pathogen for all parties involved. With the recent relaxation of HIPAA requirements, multiple real-time audio and video programs are available for ophthalmologists’ use. This article discusses practical pointers to keep in mind when using telemedicine.
DOCUMENTATION
When conducting a virtual patient visit, the provider should document:
- The patient’s verbal consent to discuss his or her health information;
- The length of the virtual visit;
- The date and time of the virtual visit, down to the minute;
- The content of the virtual visit, as if the patient were sitting in the office chair; and
- Whether the visit was conducted via telemedicine (with real-time audio and video) or by phone call (audio only).
BILLING REAL-TIME AUDIO-VIDEO
In ophthalmology, we are fortunate to have two choices when it comes to the code selection of an in-office examination: (1) evaluation and management (E/M) codes (99XXX) and (2) eye visit codes (92XXX). Unlike the E/M coding guidelines, eye visit codes do not specify required history elements. The guidelines simply indicate that a medical history is required, and leave it up to the provider to document what is appropriate for each patient based on his or her presenting conditions. It is expected that the medical history will be commensurate with the patient’s overall health and presenting conditions. E/M coding requires more documentation than most ophthalmologists are used to, as the note must include history, examination, and medical decision-making. For guidance on E/M coding, visit cms.gov.1
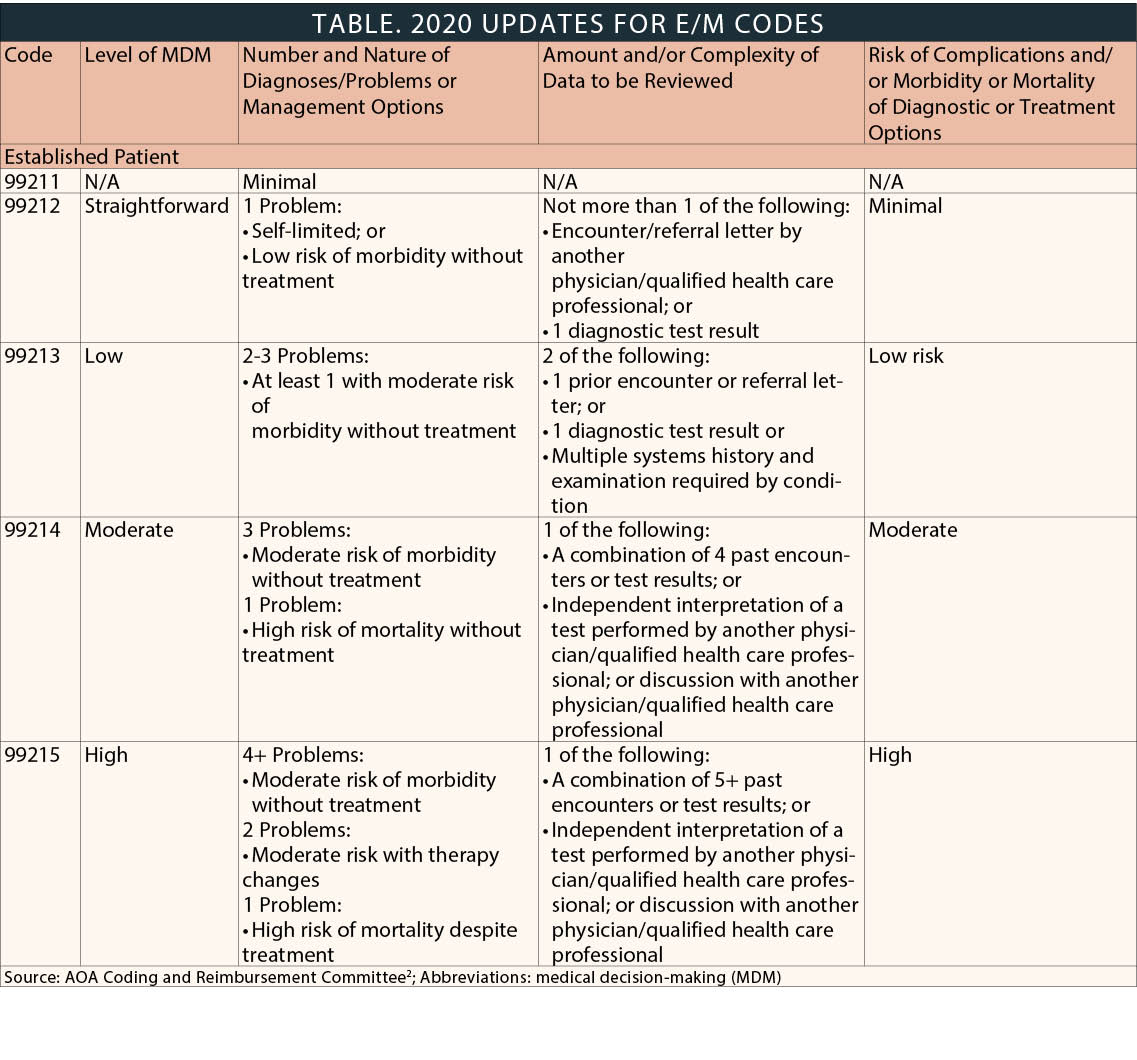
When billing real-time audio and video, a provider should not use eye visit codes because they are not approved for telemedicine consultations. E/M codes should be used instead (Table). For place of service, CMS is instructing physicians and practitioners who bill for Medicare telehealth services to report the POS code that would have been reported had the service been furnished in person (ie, Office: 11).
SHORT-TERM SOLUTIONS
Non–HIPAA-compliant platforms may serve as sufficient short-term telemedicine solutions. However, I suspect that many patients will grow accustomed to these virtual interactions, so physicians may want to opt for a program with greater security that can be used over a longer term.
Skype. Although Skype has been in use for years, the platform offers more capabilities than most users realize. Skype enables not only video-based visits but also messaging and file sharing. Further, patients who use Skype to connect with their physicians need an email account to sign up, making the platform more secure than some others. Additionally, the program works from a desktop or a smartphone, which is a big advantage. The one downside is that using Skype may give a patient unfettered access to his or her physician, which can present challenges.
Google Hangouts. Google Hangouts has the same pros and cons as Skype. The program works seamlessly when used with individuals who have Google accounts. Plus, I find the Google Hangouts user interface easier to interact with than Skype’s. Platforms such as Zoom and BlueJeans present similar challenges as Skype and Google Hangouts.
It is also important to note that, if a patient wishes to talk to his or her physician using one of these platforms, a substantial amount of back and forth is required to schedule the virtual visit and ensure proper configuration.
HIPAA-COMPLIANT PLATFORMS
Doxy.me. Doxy.me is a popular HIPAA-compliant telemedicine platform, primarily because it is free. The user interface is bare-bones—it entails the doctor talking with the patient with no frills, which I think is a benefit. One caveat: Upon logging in, a patient can enter any name he or she wants, so there is no way to verify if the virtual visit is indeed coming from the intended patient. Doxy.me provides a timestamp at the end, which the physician has to manually enter into his or her note. It is important to note that the data are not stored and therefore cannot be accessed in the event of an audit.
Paid services. Several paid services allow seamless connection with patients, document call length and duration, control who initiates the call, and give providers the ability to make themselves unavailable. Paid services also provide dedicated support, depending on the service.
Video | Ophthalmologists walk through virtual patient consultations using different telemedicine platforms.
TELEMEDICINE ETIQUETTE
When conducting a virtual patient visit, the following telemedicine etiquette tips are advisable.
- Work in a quiet space.
- Be aware of your surroundings. Patients will see whatever is behind you, unless you are using Skype, which can blur out the background. I suggest sitting in front of a blank wall.
- Facial expressions matter and will be the patient’s primary focus. Smile: You’re on camera.
- Wear a presentable shirt and consider your physical appearance.
- Speak louder than usual. The audio may be worse than in a real-world setting.
- Use a headset. Simple earbuds with a microphone are adequate.
CONCLUSION
Having experimented with telemedicine for years and testing every available platform, I recommend utilizing a HIPAA-compliant paid program. The prices for most services are not excessive, and the capabilities and security afforded far outweigh the cost. Keep in mind that whichever service you choose should offer a streamlined process for you, your staff, and your patients. The easier a platform is to use, the better the experience will be for all involved.
1. Evaluation and Management services. Centers for Medicare & Medicaid Services. www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/eval-mgmt-serv-guide-ICN006764.pdf
2. CPT and E&M updates for 2020 and beyond. AOA Coding and Reimbursement Committee. www.aoa.org/assets/documents/sgrc-tpc/handouts%20em%2020-21%20sgrc-tpc%20meeting.pdf.
