


The retina space has evolved tremendously since I was in fellowship training and since my early days of practice. This article overviews five technologies and treatments that have majorly advanced retina care and continue to benefit patients today.
1. OCT. Arguably the number-one evolution in retina over the past 10-plus years is OCT imaging. OCT has fundamentally changed all aspects of practice for retina specialists, starting with the way in which we visualize the posterior segment. In the past, flat contact lenses were used to analyze the macula and scrutinize whether edema was present; with this two-dimensional imaging approach, clinical examination was challenging and time-consuming.
Today, retina specialists primarily use OCT to (1) make a diagnosis and (2) judge a treatment response, be it to anti-VEGF therapy or surgery. Educating patients about their OCT findings is critical to helping them understand their disease and their treatment. OCT has also enabled retina specialists to visualize morphological changes and better understand various stages of diseases, such as vitreomacular traction, and to make improved diagnoses as a result.
Not only has OCT fundamentally changed clinical care, but it has also revolutionized practice workflow. When I started practice, OCT had not yet been widely adopted. Our traditional flow of patients went from optometry, to general ophthalmology, and then to retina. With the implementation of OCT, we have found that optometrists see the retina as well as we do, so they are able to make subtle diagnoses and send patients directly to us. Now, when patients are referred in from optometry colleagues, we usually refer them back for optometric care. When we are referred patients from general ophthalmology colleagues, we refer them back for cataract care. OCT has been a game changer in our referral patterns and in how we educate our referrals.
Going forward, advances in OCT imaging will enhance the speed at which we perform diagnostic testing and the detail of the images captured. Swept-source OCT imaging, for example, enables a faster scan speed that other OCT techniques, providing faster acquisition of images. In the future, we will likely be able to obtain much wider fields of view with OCT, which will enable us to stop using fluorescein angiography.
2. Anti-VEGF therapy. Around the time that I was finishing fellowship, the FDA approved ranibizumab (Lucentis, Genentech) for the treatment of classic and occult wet age-related macular degeneration (AMD), making it the first anti-VEGF agent available for this indication. Around this time, retina specialists also started using bevacizumab (Avastin) off label for wet AMD. Bevacizumab is still the most commonly injected medication into the eye and will likely continue to be because of its economic advantage over ranibizumab.
Upon the introduction of anti-VEGF therapy into retina, unprecedented visual gains were seen. Several clinical trials substantiated the use of these agents, and additional innovation and regulatory approvals were seen in the anti-VEGF space. For those interested in the full history of anti-VEGF therapy in retina care, the New Retina Radio podcast has a fantastic three-part series dedicated to this topic (see Listen Up).

3. Small-gauge surgery. Small-gauge surgery has done to retina surgery what phacoemulsification has done to cataract surgery. It is a real difference maker and is continuing to evolve, with the latest iteration being 27-gauge surgery. Small-gauge retina surgery increases the speed of our procedures as well as the healing time.
In addition to small-gauge surgery, there has been a variety of other complementary evolutions, including valved cannulas, which allow safer surgery, as well as dual-blade cutters, which allow cutting speeds of up to 20,000 cuts per minute, enabling safer and more effective surgery. These advances have also expanded our surgical scope, as they can be used to perform more difficult procedures.
The removal of vitreous opacities has become the second most common surgery performed in our practice, after epiretinal membrane surgery. Sometimes these patients come in after premium IOL surgery and describe feeling like a screen door is between them and their best vision. Small-gauge vitrectomy is a safe and effective way to address this. The removal of vitreous opacities can have a dramatic effect on patients’ quality of life, as they have been reported to decrease contrast sensitivity by 50%.1 Not unsurprisingly, successful surgery in one eye leads to treatment of the fellow eye in more than 70% of cases. In our practice, these individuals end up being our happiest patients postoperatively.
4. 3D heads-up surgery. Heads-up 3D surgery technology has given us a tremendous ability to educate referring doctors with a unique and hands-on approach. Typically, in our OR, not a day goes by that we don’t have observers, either from industry, from ophthalmology, or from optometry; 3D heads-up visualization has revolutionized the way in which we educate those observing our retina surgeries.
5. Port delivery system. The Port Delivery System (Genentech; not yet approved) is a durable drug reservoir designed to dispense ranibizumab over time after surgical implantation (Figure). The device is placed in about a 30-minute procedure, and subsequent refills are performed in office. The device is currently under investigation; topline results of the phase 3 ARCHWAY trial indicated noninferior and equivalent efficacy on a 6-month refill protocol compared with monthly ranibizumab injections. Full results will be reported later this year.
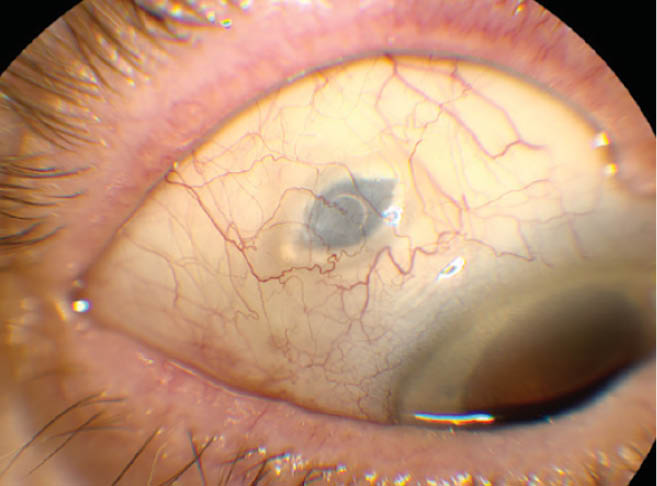
Figure | External 1-month postoperative photograph of the Port Delivery System in the LADDER study. Reprinted with permission from Samir PN, Jenkins TL, Pieramici DJ, Regillo CD. Use of the Port Delivery System in AMD. Retina Today. May/June 2019.
Eye care providers who administer or refer patients for anti-VEGF therapy know that patients’ number-one complaint is having to come back to the office every month. With this technology, we hope to ultimately be able to refill the reservoir once or twice a year, thereby dramatically decreasing the required number of office visits and reducing the treatment burden, making it a real game changer for patients and providers alike.
1. Sebag J, Yee KMP, Nguyen JH, Nguyen-Cuu J. Long-term safety and efficacy of limited vitrectomy for vision degrading vitreopathy resulting from vitreous floaters. Ophthalmology. 2018;2(9):881-887.
