
Unilateral or bilateral limbal stem cell deficiency (LSCD) is a significant cause of vision loss in children and adults. Many techniques and advances have been developed since José Barraquer, MD, presented his first case of successful limbal and conjunctival transplantation in 1964.
Standard nomenclature for limbal stem cell transplant techniques depends on the source of donor tissue, the carrier tissue, and whether the donor tissue is conjunctival or limbal. Techniques that use autografts from the healthy fellow eye are indicated in unilateral LSCD. These include conjunctival-limbal autograft (CLAU), cultivated limbal epithelial transplant (CLET), and simple limbal epithelial transplant (SLET). For bilateral disease, the donor can be from a cadaver graft (keratolimbal allograft) or a living relative (living-related conjunctival limbal allograft).
Pioneered by Virender Sangwan, MS, SLET is the newest technique to address LSCD.1 The procedure involves transplanting a small area of limbal tissue from the patient’s healthy fellow eye onto an amniotic membrane scaffold that is affixed to the recipient eye. This allows the donor stem cells to repopulate the corneal epithelium of the recipient (Figure). According to Ali Djalilian, MD, director of the Stem Cell Therapy and Corneal Tissue Engineering Laboratory at Illinois Eye and Ear Infirmary, in addition to providing stem cells, SLET creates “a healthier environment for the [host] stem cells that survived the injury to come back.”
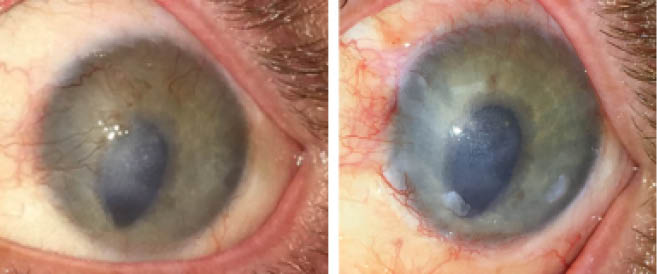
Figure. After LASIK, this eye sustained an alkali injury. Flap necrosis and neovascularization encroaching on the central visual axis were evident (left). The necrotic area was amputated, and SLET was performed, with transplants placed peripherally. Central neovascularization had improved 1.5 years after SLET (right).
Courtesy of Ali Djalilian, MD
SURGICAL TECHNIQUE
The 2012 article by Sangwan et al presenting SLET described six patients with unilateral total LSCD from chemical injury who underwent the procedure.1 All patients achieved an epithelialized corneal surface by 6 weeks and remained stable for a mean follow-up time of 9 months.
In SLET, a 2 x 2–mm strip of superior limbal tissue, incorporating 1 mm of clear cornea, is harvested from the donor eye (the healthy fellow eye). A 360º peritomy and superficial keratectomy are performed to remove abnormal pannus in the recipient eye. Next, the recipient cornea is covered with amniotic membrane using fibrin glue. The donor graft is cut into eight to 10 pieces with Vannas scissors. The cut fragments are secured over the paracentral cornea with fibrin glue, and the cornea is covered with a bandage contact lens. Antibiotic and steroid drops are initiated, and the steroid is tapered over 6 weeks in both eyes. The bandage contact lens is removed after 7 days.
INDICATIONS FOR SLET
Because SLET usually involves harvesting limbal cells from the healthy fellow eye, the procedure is typically performed for unilateral disease such as chemical and thermal burns. Other less common indications include surface reconstruction during excision of pterygium and ocular surface squamous neoplasia. Contraindications include bilateral causes of LSCD such as contact lens–induced LSCD, Stevens-Johnson syndrome, aniridia, and ocular cicatricial pemphigoid.
Basu and colleagues reported long-term follow-up of 125 patients who underwent SLET for unilateral total LSCD from chemical injury. Patients were observed for a median of 1.5 years.2 The investigators found that 76% of patients maintained an epithelialized avascular cornea at follow-up and 75% experienced a 2-line improvement in BCVA. None of the donor eyes demonstrated LSCD or other complications.
COMPARISONS WITH OTHER TECHNIQUES
Compared with other conventional methods that require a living relative donor or deceased donor, SLET obviates the need for long-term systemic immunosuppression and reduces the risk of rejection. Additionally, the procedure requires less tissue to be harvested from the donor eye compared to CLAU. In SLET, only 2 to 3 mm2 of limbal tissue are harvested from the donor eye, whereas CLAU requires approximately 4 clock hours of tissue. CLET also allows less tissue to be explanted from the donor eye than in CLAU, but the ex vivo expansion of limbal stem cells necessary in CLET is costly because it requires a laboratory to culture the stem cells for 10 to 14 days. Moreover, CLET entails two surgeries—one to harvest the stem cells and one for implantation.
CLAU was developed in 1989, and 30 years of long-term data demonstrate its safety and efficacy. More long-term data are required for SLET, but studies comparing the procedure with established techniques have been favorable. Dr. Sangwan told us that he would prefer CLAU over SLET for an eye with extensive symblepharon or conjunctival disease.
Shanbhag and colleagues conducted a systematic literature review comparing SLET, CLAU, and CLET.3 The review included 22 case series and a total of 1,023 eyes. A majority of the patients underwent these procedures for ocular burns (88%). CLAU, CLET, and SLET had success rates of approximately 81%, 61.4%, and 78%, respectively, for creating an epithelialized, stable, avascular corneal surface. Improvements in BCVA were 74.4%, 51.5%, and 68.6% for CLAU, CLET, and SLET, respectively. Despite these promising findings for SLET, randomized clinical trials are needed to compare its efficacy to that of CLAU and CLET.
COMPLICATIONS AND DRAWBACKS
Complications of SLET include infectious keratitis, corneal melt, and failure. According to Basu et al, several factors were associated with failure: acid injury, severe symblepharon, SLET with concurrent keratoplasty, and postoperative loss of transplants.2 Gupta et al reported a corneal graft survival rate of 85% at 6 months in seven patients who underwent penetrating keratoplasty (PKP) an average of 9.5 months after SLET.4
Dr. Sangwan cautioned against performing PKP and SLET concurrently. If a patient requires both procedures, he recommended performing SLET first, followed by PKP at a later date if SLET is successful.
CONCLUSION
SLET is a viable option for patients with unilateral LSCD. The procedure offers advantages compared to CLAU and CLET, but longer-term follow-up is required.
1. Sangwan VS, Basu S, MacNeil S, Balasubramanian D. Simple limbal epithelial transplantation (SLET): a novel surgical technique for the treatment of unilateral limbal stem cell deficiency. Br J Ophthalmol. 2012;96(7):931-934.
2. Basu S, Sureka SP, Shanbhag SS, et al. Simple limbal epithelial transplantation: long-term clinical outcomes in 125 cases of unilateral chronic ocular surface burns. Ophthalmology. 2016;123(5):1000-1010.
3. Shanbhag SS, Nikpoor N, Rao Donthineni P, et al. Autologous limbal stem cell transplantation: a systematic review of clinical outcomes with different surgical techniques [published online ahead of print May 22, 2019]. Br J Ophthalmol. doi: 10.1136/bjophthalmol-2019-314081.
4. Gupta N, Farooqui JH, Patel N, Mathur U. Early results of penetrating keratoplasty in patients with unilateral chemical injury after simple limbal epithelial transplantation. Cornea. 2018;37(10):1249-1254.

